

Cipher
Administrator
- Messages
- 1,429
I wrote a post about VNS in another thread regarding its effects on GABA, thought it might belong in this thread as well:
----
Vagus nerve stimulation seems to increase GABA in the brain. Here's a study that compared GABAa receptor density in people with epilepsy before and 1 year after the implantation of a VNS (vagus nerve stimulation) device. The VNS group had an increase of 42,5 % in GABAa receptor density and the control group had an increase of 7,6 %. This might only apply on people with epilepsy , but there are studies indicating a GABA enhancing effect in healthy individuals also (like this study; "SICI, a double-pulse TMS paradigm informative of GABA-A activity, was significantly increased in right motor cortex after real tVNS."). I've read that the anti-epileptic effects of VNS takes some time to manifest, so that might also apply to the GABA increasing effect. "Unlike drugs, where efficacy may decline with time, efficacy with VNS continues to improve over a period of 18 months to 2 years." (source)
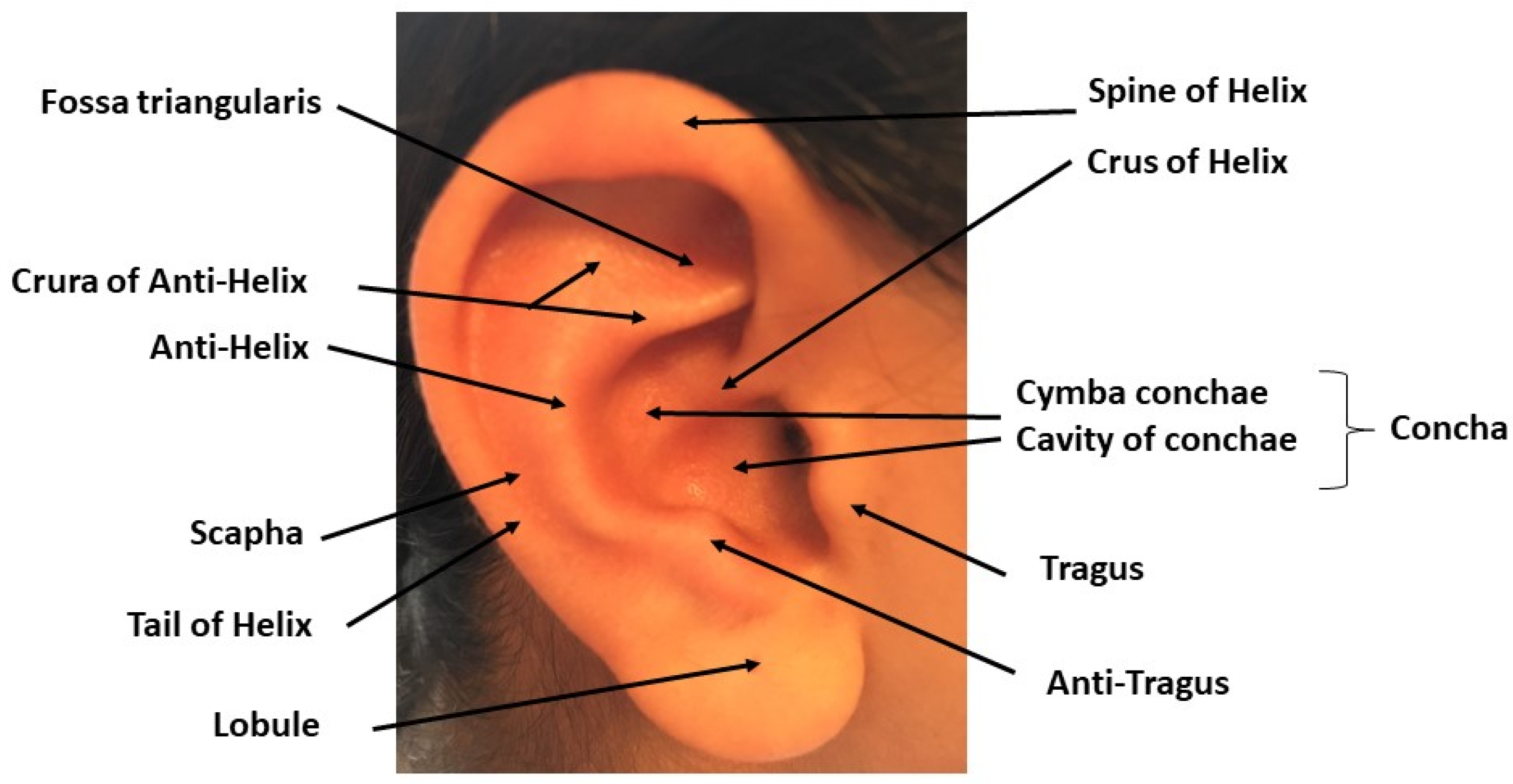
"Regular" VNS is achieved using a neurostimulator that's surgically-implanted in the chest. An alternative, noninvasive form of VNS is called Transcutaneous Vagus Nerve Stimulation (tVNS), alternatively Transcutaneous Auricular Vagus Nerve Stimulation (taVNS). This can be achieved using a TENS/EMS machine and an ear electrode. VNS have also been shown to lower inflammation, for example in this pilot study with rheumatoid arthritis. I have myself just started experimenting with taVNS using a Beurer EM 49 and an earclip stimulating the tragus.
There is a couple of parameters that is relevant when it comes to VNS; current intensity, frequency (Hz), pulse width (μs), duty cycle (On/Off time) and session duration. NEMOS, which is a tVNS-device used for epilepsy, uses 25 Hz, 250 μs pulse width, 30s ON, 30 OFF duty cycle in 1 hour sessions, 4 sessions per day. This is a lot different from the parameters used in the rheumatoid arthritis study, where they used 10 Hz, 250 μs pulse width, 60 seconds per session, 4 sessions per day. 4 minutes instead of 4 hours! The field is still in its infancy, so parameters varies greatly and what's optimal is not known. According to this study lower frequencies (≤10 Hz) are better suited for anti-inflammatory purposes, and higher frequencies (20-30 Hz) are better suited for epilepsy and depression.
When it comes to current intensity it seems like what's the most common is to adjust the intensity to a bit above the perceptual threshold. Perceptual threshold means the lowest current that's noticeable. According to this paper 200 % of the perceptual threshold is appropriate.
Parameters used with epilepsy might be better for increasing GABA in the brain. I don't know if lower frequencies (≤10 Hz) increases GABA in the brain. Also as a side-note; because VNS stimulates the "cholinergic anti-inflammatory pathway", it might be prudent to combine this with an adequate choline intake, using choline bitartrate for example. But that's just pure speculation on my part.
----
Vagus nerve stimulation seems to increase GABA in the brain. Here's a study that compared GABAa receptor density in people with epilepsy before and 1 year after the implantation of a VNS (vagus nerve stimulation) device. The VNS group had an increase of 42,5 % in GABAa receptor density and the control group had an increase of 7,6 %. This might only apply on people with epilepsy , but there are studies indicating a GABA enhancing effect in healthy individuals also (like this study; "SICI, a double-pulse TMS paradigm informative of GABA-A activity, was significantly increased in right motor cortex after real tVNS."). I've read that the anti-epileptic effects of VNS takes some time to manifest, so that might also apply to the GABA increasing effect. "Unlike drugs, where efficacy may decline with time, efficacy with VNS continues to improve over a period of 18 months to 2 years." (source)
"Regular" VNS is achieved using a neurostimulator that's surgically-implanted in the chest. An alternative, noninvasive form of VNS is called Transcutaneous Vagus Nerve Stimulation (tVNS), alternatively Transcutaneous Auricular Vagus Nerve Stimulation (taVNS). This can be achieved using a TENS/EMS machine and an ear electrode. VNS have also been shown to lower inflammation, for example in this pilot study with rheumatoid arthritis. I have myself just started experimenting with taVNS using a Beurer EM 49 and an earclip stimulating the tragus.
There is a couple of parameters that is relevant when it comes to VNS; current intensity, frequency (Hz), pulse width (μs), duty cycle (On/Off time) and session duration. NEMOS, which is a tVNS-device used for epilepsy, uses 25 Hz, 250 μs pulse width, 30s ON, 30 OFF duty cycle in 1 hour sessions, 4 sessions per day. This is a lot different from the parameters used in the rheumatoid arthritis study, where they used 10 Hz, 250 μs pulse width, 60 seconds per session, 4 sessions per day. 4 minutes instead of 4 hours! The field is still in its infancy, so parameters varies greatly and what's optimal is not known. According to this study lower frequencies (≤10 Hz) are better suited for anti-inflammatory purposes, and higher frequencies (20-30 Hz) are better suited for epilepsy and depression.
When it comes to current intensity it seems like what's the most common is to adjust the intensity to a bit above the perceptual threshold. Perceptual threshold means the lowest current that's noticeable. According to this paper 200 % of the perceptual threshold is appropriate.
Parameters used with epilepsy might be better for increasing GABA in the brain. I don't know if lower frequencies (≤10 Hz) increases GABA in the brain. Also as a side-note; because VNS stimulates the "cholinergic anti-inflammatory pathway", it might be prudent to combine this with an adequate choline intake, using choline bitartrate for example. But that's just pure speculation on my part.




")