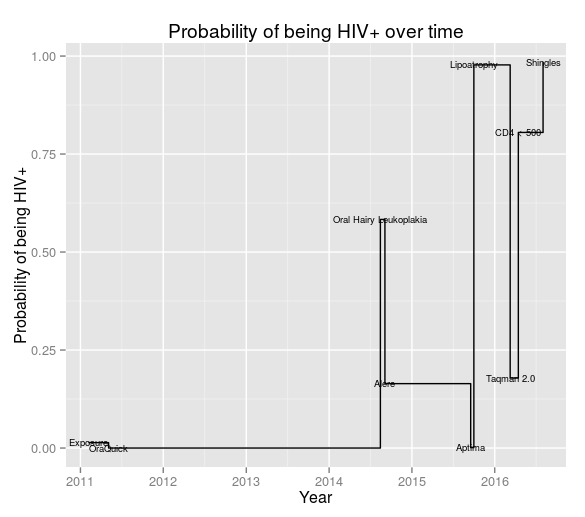
Is there a reason you suspect HIV over any particular virus? I assume you have been in close contact with a person who carries HIV shortly before the sickness period started? Otherwise HIV seems exceedingly unlikely, given the negative test results and the way it only transmits through close contact.
CFS/ME patients are often documented with various immune deficiencies, which have nothing to do with HIV or any retrovirus. In tests on CFS/ME patients, a number of viruses have been identified, but there isn't a consistent pattern linking the disease to any certain virus. The strongest case is for enteroviruses, which Dr Chia have identified from stomach biopsies of CFS/ME patients (
link).
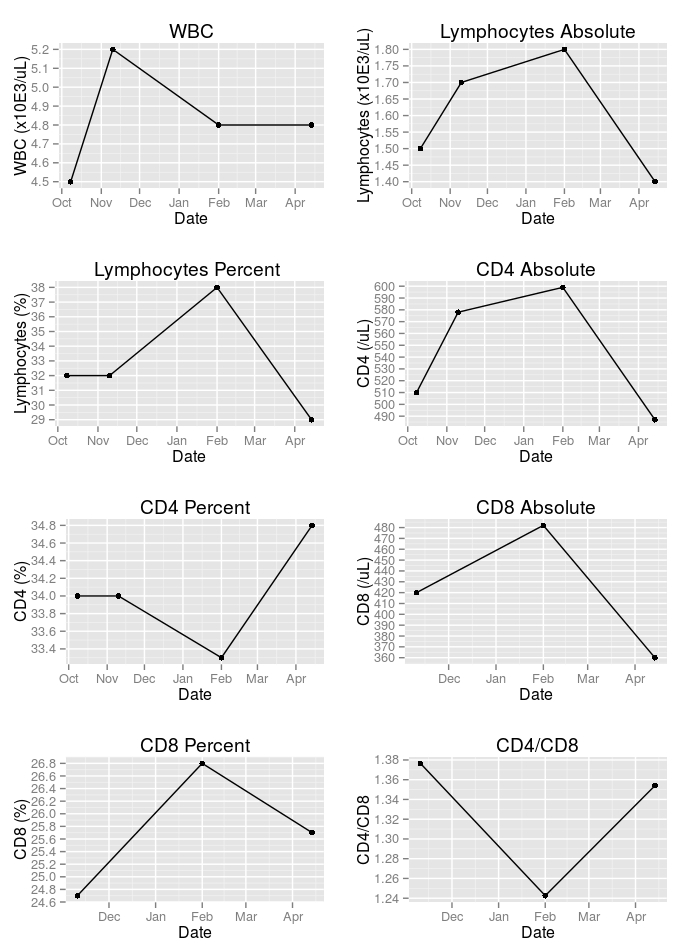
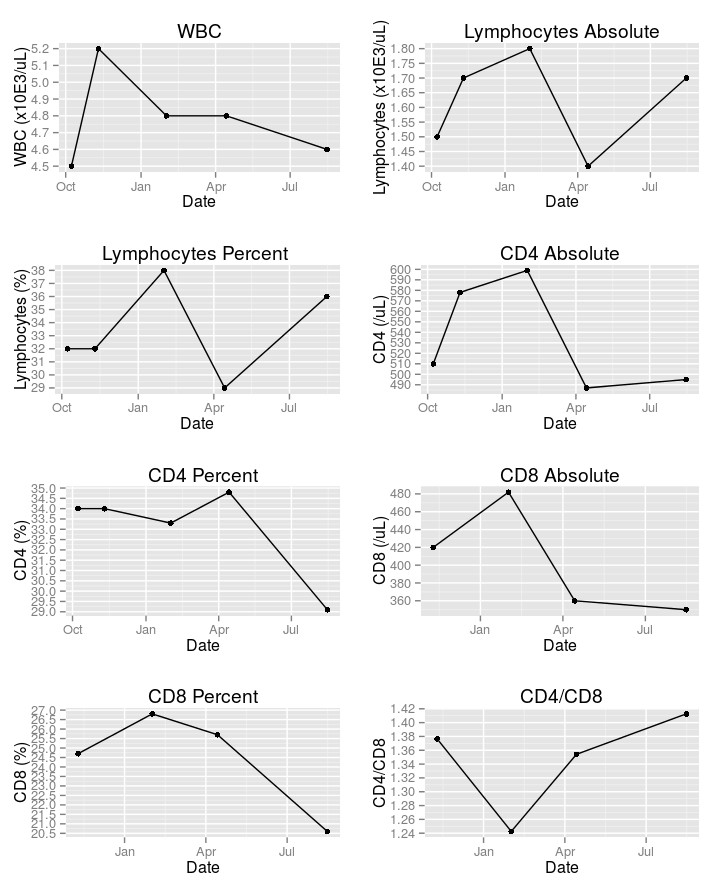
I have had a lowish WBC count and other slight abnormalities on a number of tests over the last 10 years, eye floaters, nerve pain, a constant feeling of sickness, etc. A very low ESR is also commonly found among CFS/ME patients on this forum, it is suspected this is due to hypercoagulation of blood. These are all common symptoms with CFS/ME and have nothing to do with HIV specifically.