

undiagnosed
Senior Member
- Messages
- 246
- Location
- United States
Diagnosis of HIV is determined in the context of test results, transmission risk history, and symptoms. While HIV test results to date have all been negative, symptoms and secondary lab tests provide strong evidence supporting the HIV+ hypothesis. Using Bayesian inference, the probability of being HIV+ was calculated over time for each new piece of available evidence. Based on all of the evidence to date, the most recent probability of being HIV+ was determined to be 95.3%. The graph below shows the latest calculated probabilities which have changed a little from the last post due to some adjustments to some of the numbers.
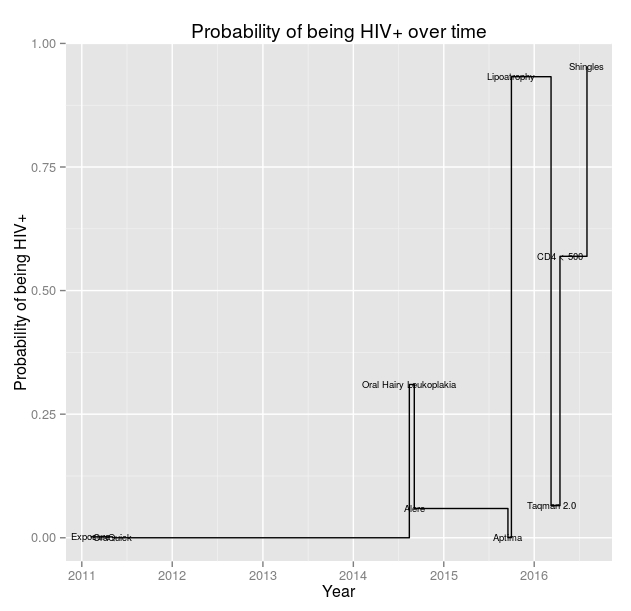 The latest probability of being HIV+ was calculated given the negative Oraquick ADVANCE result, negative Alere Determine result, negative Aptima Gen-probe result, negative Taqman 2.0 result, Oral Hairy Leukoplakia symptom, lipoatrophy symptom, CD4 < 500 result, shingles symptom, and risk history. The updated paper contains all of the calculation details. If anyone has skills in statistics and would like to review my work, I would appreciate it.
The latest probability of being HIV+ was calculated given the negative Oraquick ADVANCE result, negative Alere Determine result, negative Aptima Gen-probe result, negative Taqman 2.0 result, Oral Hairy Leukoplakia symptom, lipoatrophy symptom, CD4 < 500 result, shingles symptom, and risk history. The updated paper contains all of the calculation details. If anyone has skills in statistics and would like to review my work, I would appreciate it.
")