The following text describes my backup antiretroviral (ARV) treatment plan. It's a long read that outlines some of my thoughts and investigations. If anyone has any feedback on any part of it, let me know. I'm going to have some difficult decisions to make.
My goal is and always has been to get a definitive diagnosis. I suspect based on
evidence to date a retroviral infection is causing my symptoms, specifically some type of HIV. While clinically available tests I've taken have been negative, I have not been able to get access to less specific research assays that would be able to detect divergent virus. I've been pursuing multiple avenues including trying to work with researchers, contract research organizations, and even designing my own assays. However, this process has had many setbacks and is taking too long. I think ultimately I'm going to run out of time before I'm able to get a definitive diagnosis. Therefore, I am formulating a treatment plan that I can execute on my own if things get much worse.
Based on my research, my ideal combination of ARVs would be Descovy (emtricitabine and tenofovir alafenamide) and Tivicay (dolutegravir). This combination contains two nucleoside reverse transcriptase inhibitors (NRTI) and an integrase strand transfer inhibitor (INSTI). It is a first line HIV-1 treatment and has some advantages over Genvoya which is another popular first line HIV-1 treatment. Descovy + Tivicay contains 3 drugs, one less than Genvoya which has a boosting agent that can interact with other medications.
However, no generic version of Descovy exists so it is unaffordable without insurance coverage or other financial assistance. Since I cannot get a diagnosis, those options are off the table. Additionally, without a generic available, it would be more difficult to find a pharmacy willing to sell it without a prescription. The available alternative is Truvada (emtricitabine and tenofovir disoproxil fumarate) or one of the many Truvada generics that exist. This formulation is known to have more significant kidney and bone toxicity than Descovy, but is widely available at affordable prices. Tivicay now also has a generic version available in India that is affordable.
For some cost comparisons, I looked at Descovy + Tivicay costs through online pharmacies vs. Tenvir-EM (Truvada generic) + Instgra (Tivicay generic). In the US, Truvada can be prescribed as Pre-exposure prophylaxis (PrEP) for people at risk for acquiring HIV, but the hassle involved would likely not be worth it in my case.
Preferred ARVs
Descovy
30 pills (1 month) - $1112.36
Canada Drugs
Tivicay
30 pills (1 month) - $771.44
Canada Drugs
Total per month
$1883.80 + shipping (requires prescription)
Generic ARVs
Tenvir-EM
30 pills (1 month) - $55.50 + $25.00 shipping = $80.50
ALLDAYCHEMIST
Instgra
30 pills (1 month) - $60 + $30 shipping = $90.00
IndiaMart Supplier
Total per month
$170.50
The generic ARVs are an order of magnitude cheaper and within the realm of my financial constraints. However, there are a number of risks to consider if self-treatment with these ARVs is performed and I do not take them lightly.
Risks
1. Drug quality unknown, manufactured in India, sold by independent vendors
The possible issues with drug quality include contamination, fake drugs (possibly dangerous), and not the correct levels of drug. Any of these issues could be very serious. Contamination or other unknown ingredients could be toxic and cause illness or even death in the most extreme case. Incorrect levels of the drug could lead to resistant virus which would be more difficult to treat and require possibly more toxic ARVs. It is therefore very important to have a high degree of confidence that the drug is legitimate and as claimed. This means that the manufacturer is producing a trustworthy drug and that the vendor is sourcing the drug directly from the manufacturer.
The manufacturer of Tenvir-EM is Cipla, an Indian pharmaceutical company. Cipla got tentative approval from the FDA for Tenvir-EM in
2014. Tentative FDA approval is defined as follows:
FDA reviews the marketing applications using its normal standards for authorization. If the product still has marketing protection in the U.S., FDA issues a "tentative approval" rather than a "full" approval. The "tentative" approval signifies that the product meets all safety, efficacy, and manufacturing quality standards for marketing in the U.S., and, but for the legal market protection, it would be on the U.S. market.
So there is good evidence that Tenvir-EM manufactured by Cipla is legitimate and safe. The next piece is to make sure that the vendor you purchase it from is sourcing it directly from the manufacturer. This is more difficult to establish. However, there is a group in the UK who have imported Tenvir-EM from particular vendors and performed Therapeutic drug monitoring (TDM) on themselves. This process measures medication concentrations in the blood. Testing
showed adequate blood drug levels demonstrating that the drugs purchased were legitimate. So by ordering from one of the listed vendors, there is reasonable assurance that a legitimate drug will be received.
The situation with dolutegravir is less certain. The only dolutegravir with tentative FDA approval to date is manufactured by Aurobindo Pharma. However, I was unable to find any vendors for this drug. The manufacturer for Instgra is Emcure. While Instgra does not have FDA tentative approval for dolutegravir, they have tentative approval for a number of other ARVs. However, Emcure has also been issued
warnings from the FDA in the past for violations of good manufacturing processes. Cipla has also been warned along with many other Indian pharmaceutical manufacturers so it may not be too significant. The evidence is not as strong that Emcure is manufacturing a reliable drug, but unless an alternative can be found, it is currently the best option.
With respect to vendors, there have been no third party tests as with Tenvir-EM which is used for PrEP. Therefore trust must be established with the vendor. The vendor I communicated with provided me with a number of documents claiming their legitimacy. However, ultimately there is some risk here as a high degree of trust cannot be established.
2. Limited access to alternatives or other medications if significant sides effects are experienced
Rarely there can be significant sides effects associated with starting antiretroviral therapy. For example immune reconstitution syndrome could be experienced which may require other medications to manage. Additionally it is possible that sides effects from the first line ARVs could be intolerable and would require switching to an alternative combination. It would be difficult to manage any serious problems on my own so the only real mitigation is that statistically the likelihood of such a scenario is relatively low.
As of the end of 2015, more than
79,000 HIV- people at risk for acquiring HIV in the US take Truvada for PreP to prevent HIV infection. It is a generally well tolerated drug with minor short term side effects if any. Long term there are some known possible kidney and bone toxicities that need to be monitored. The drug has been deemed safe enough to be used for HIV prevention which is indicative of its relatively low toxicity.
A number of people on the forums here have used older generation ARVs and experienced significant side effects but reports from members using newer generation drugs such as Truvada have been that relatively minor or no side effects have been experienced. The issues I've seen reported include
@Daffodil who took AZT and RAL for a trial and reported significant lasting side effects presumably from the AZT. Another case was
@PhoenixBurger who took a 30 day Post Exposure Prophylaxis (PEP) combination consisting of AZT, Lamuvidine, Ritonivir, and Lopinavir.
@PhoenixBurger reported the onset of CFS symptoms after this course of medications. AZT and a hefty combination of other old NRTIs and protease inhibitors are known to have more significant side effects than newer class ARVs.
@ScottTriGuy who has taken various ARVs for treatment of HIV has reported minor side effects from his newer ARVs, but issues including significant nausea when he was taking AZT early on.
@cornwellsb has been taking Truvada for PrEP which has been well tolerated.
Truvada includes 2 NRTIs and as previously described is generally well tolerated. I would also be adding 1 INSTI to complete the combination for treatment of HIV rather than PrEP. Dolutegravir is also generally well tolerated. Given the general tolerability, there is a decent chance of not needing to switch medications due to side effects or toxicities.
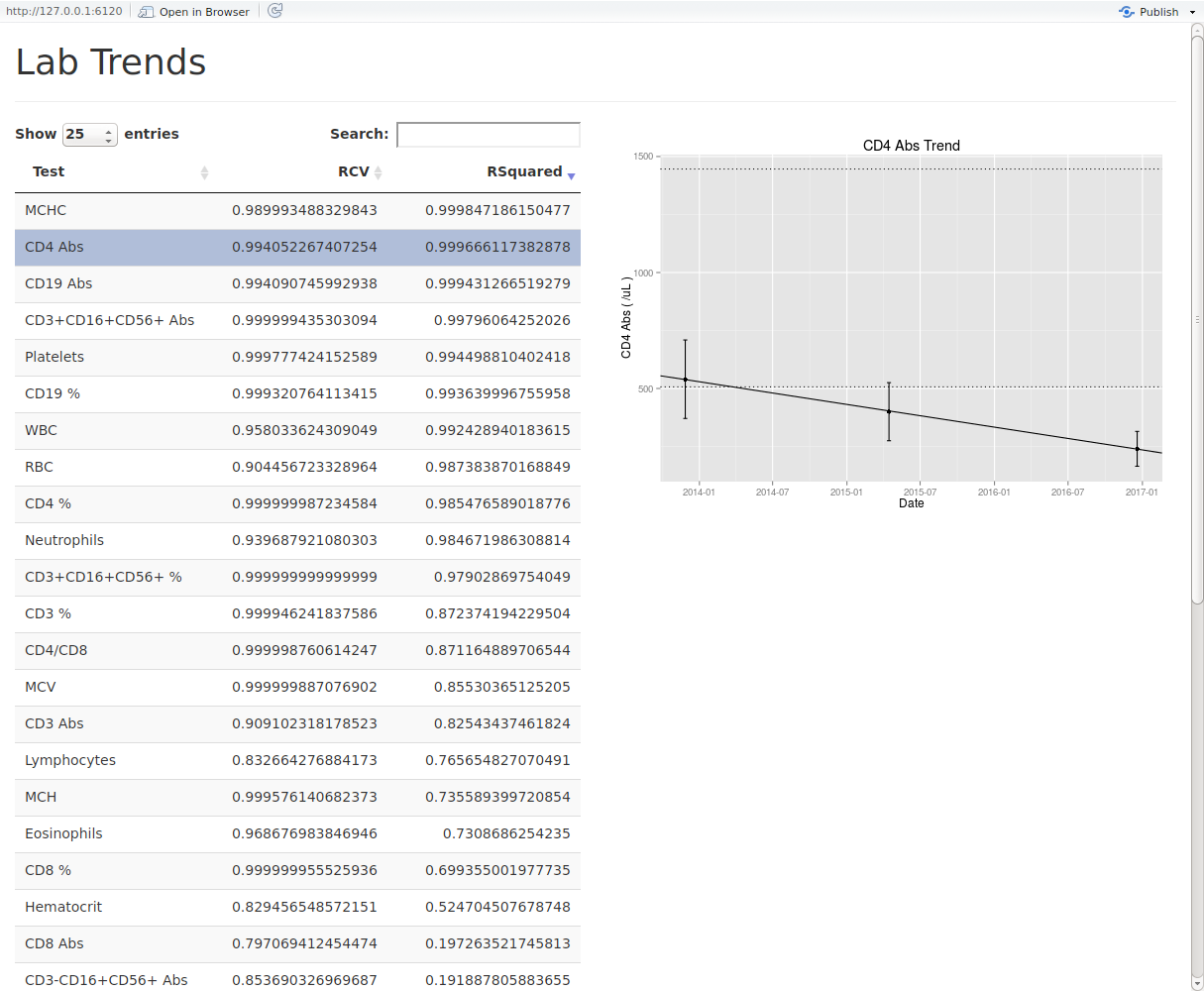
3. Can't monitor viral load, have to use CD4 and clinical indications as markers
This is a major sticking point. Since none of the clinically available viral load monitoring assays used to date have detected any viral load, ARV treatment monitoring cannot be performed optimally.
The World Health Organization recommends use of clinical and/or immunological monitoring (CD4 count) if viral load testing is not available. This is typically done in resource-limited countries where viral load testing is not available. There are significant problems with this approach. It has been found that misclassifications of treatment failure has been as high as
50%. This means medications can be switched unnecessarily even though the viral load is suppressed or that significant resistance can be developed due to not knowing that the viral load is not suppressed.
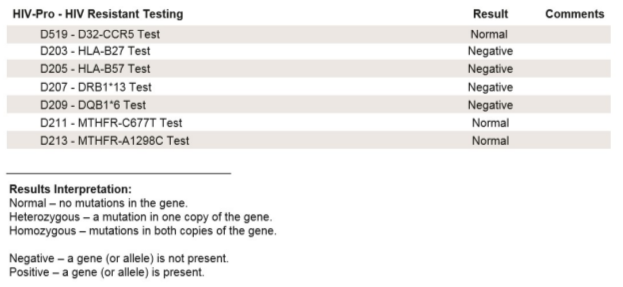
4. Don't know resistance profile, possible intrinsic resistance e.g. HIV-2
Given that none of the common epidemic strains of HIV could be detected with clinically available tests taken to date, it is unknown what type could be implicated. However, some of the evidence makes HIV-2 look more likely. This is because more extensive testing for HIV-1 has been performed and the presence of some immune characteristics such as CD4/CD8 > 1, 6 years after infection. The main thing going against this is the low reported prevalence in the US. Another possibility is a recombinant or rare type of HIV-1.
U.S. guidelines say that as long as you use an integrase inhibitor or protease inhibitor (rather than an NNRTI), you can start ART while waiting for the genotype results. This is one reason we can now consider “rapid starts,” sometimes on the day of diagnosis.
Using 2 NRTIs and an INSTI are generally a good choice in accordance with the statement above for treating HIV-1 in the US. Therefore, the probability of having resistance to this combination off the bat is low.
HIV-2 is intrinsically resistant to non-nucleoside reverse transcriptase inhibitors (NNRTI). Only certain protease inhibitors have been effective against HIV-2 including saquinavir (SQV), lopinavir (LPV), and darunavir (DRV). There is evidence that 2 NRTIs and 1 INSTI is effective against HIV-2 but no trials have been completed to confirm this. There is currently a
study underway using Stribild to treat HIV-2 infection. Stribild is similar to Truvada + Tivicay. The difference is that Stribild uses a different integrase inhibitor (elvitegravir) that requires a boosting agent. The study hypothesises that Stribild will be a safe and effective treatment for HIV-2. However, no results have been posted for the study yet so there is no definitive evidence yet.
One
study reported virological response of HIV-2 to dolutegravir. While the data is limited, it's at least a promising indication that dolutegravir has action against HIV-2.
5. TDF - bone, kidney toxicity
Initial and periodic laboratory testing will be required to monitor for adverse effects of ARV treatment. Generally, a number of baseline lab tests are done prior to treatment initiation. For TDF, regular monitoring of creatinine clearance and serum phosphate are needed to assess renal function.
Additionally, it would be helpful to have baseline bone density testing done and to periodically monitor this to assess any treatment impact. I would rather minimize the possibility of both of these toxicities by using TAF instead of TDF but without access to it, I'd have to accept these TDF associated health risks.
Harm if incorrect and treated unnecessarily
- Drug toxicity related adverse events
- Unecessary medication costs
My quality of life is already fairly low. Certainly, it could be worse but having the opportunity to improve it and have the best chance for prolonged health is very appealing. Ultimately it comes down to the odds of a significant medication induced quality of life decline from my current state happening.
Harm if correct and not treated
- Continued decline of immune system and quality of life
- Development of AIDS and lifethreating infections / cancers
This is obviously an extremely harmful outcome. Given my trajectory, I believe an intervention will be needed to prevent this from occurring.
Conclusion
I would much rather go through the proper channels with access to the latest, least toxic drugs that I know are legitimate. It would be safer and I would have easier accessibility to other medications if the drugs are not tolerated well. I would also prefer to have access to a viral load assay that was able to detect the virus implicated so that ARV treatment monitoring could be performed properly. However, since I do not have those options and have no indication of having those options in the near future, I am left with trying to do the best I can with the resources available to me. Now it's a matter of deciding at what point it makes sense to take the risk, while trying to ensure it's prior to any major adverse health events due to disease progression.


") In fact, I could use your comments to catch doctors' attention
In fact, I could use your comments to catch doctors' attention