Hi
@undiagnosed.
These are the typical causes of lymphocytosis and lymphocytopenia.
Causes of increased levels of lymphocytes (lymphocytosis) - more than 3.0 × 109 / l:
* Viral infections,
* Some bacterial infections (tuberculosis, syphilis, whooping cough, leptospirosis, brucellosis, yersiniosis),
* Autoimmune connective tissue diseases (rheumatism, systemic lupus erythematosus, rheumatoid arthritis).
The causes of a decreased level of lymphocytes (lymphocytopenia) are less than 1.2 × 109 / l:
* Aplastic anemia,
* HIV infection (primarily affects a variety T-helpers),
* Some forms of tuberculosis,
* Acute infections,
* Excess of glucocorticoids.
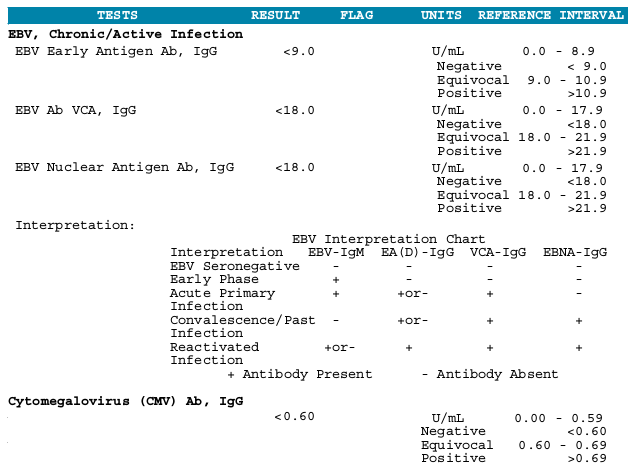
Intracellular infections (all viral infections, NOT only acute, but also chronically active) cause, first of all, relational lymphocytosis. I know very, very many of my friends suffering from chronic herpes infection having this symptom. At me it during last 20 years at least. You do not have it. In addition, I say that in most people, IgG levels to HHV4 are high, practically all cases of infectious mononucleosis were diagnosed in childhood. Most have also increased IgG titers and to HHV5. That's what I mean when I talk about patients.
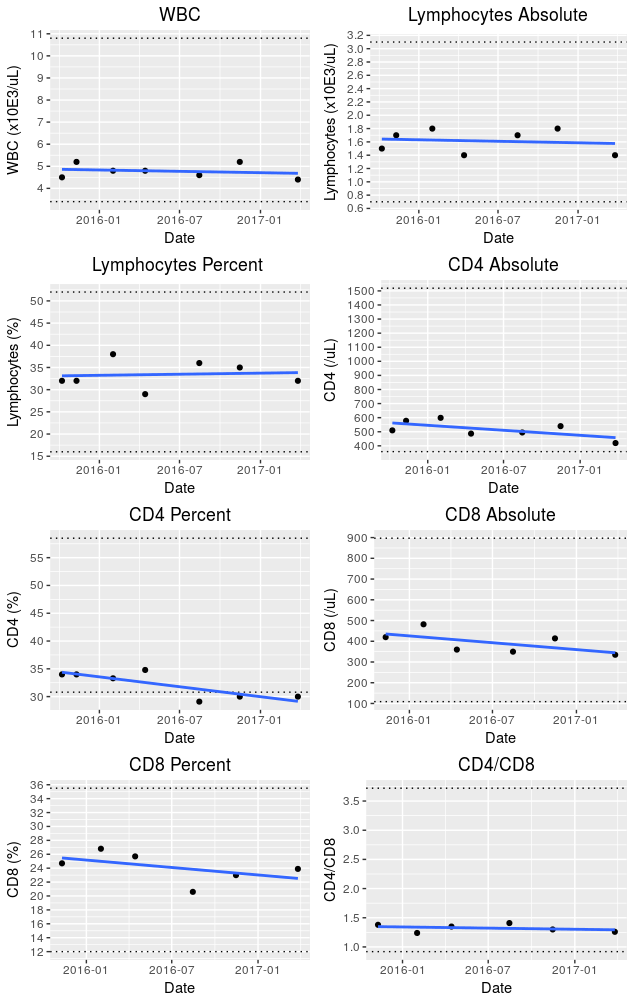
Of course, a deficit of T helper and T killers can cause lymphocytopenia, but you have it insignificant, and the trend you are talking about is statistically insignificant.
Therefore, I want to believe that you are all right.
I do not think that with your number of helpers and negative serology of HIV there are any reasons to worry.
Among the clinical manifestations of the greatest attention, in my opinion, deserves a fungal infection, most likely associated with a relatively low number of T killers.
Sincerely, ukrmen.