
No, I wasn't checked for it. It doesn't sound like I fit into it. I am being checked for periodic paralysis.Did you check for Myotonia Dystrophy? It is a multisystem/organ genetic disease that cause muscle ion channels dysfunction, fatigue, exercice intolerance, sensitivity to opioids and many drugs.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Question re: the ICC Criteria and Ion Transport issues
- Thread starter Gingergrrl
- Start date
Thought this may be of interest to some:
https://newsroom.uw.edu/news/study-reveals-why-rare-disorder-causes-sudden-paralysis
https://newsroom.uw.edu/news/study-reveals-why-rare-disorder-causes-sudden-paralysis
Gingergrrl
Senior Member
- Messages
- 16,171
@Gingergrrl In regards to the inclusion of the ion channelopathies being listed in the ICC, I can only assume that there was further input about research and clinical reports in the latter document that was not included in the earlier CCC.
That was my guess as well but I wondered what specifically they had found that led them to include it as a prominent section in the ICC but not list it in any of the other criteria?
I wish I could understand much of what you have written regarding your own particular treatment of the autoimmune condition. Maybe all of us with POTS have the autoimmunity. I will have to go back and read what your treatment is.
I apologize that my story is spread throughout thousands of posts from mid-2014 to the present (so please don't worry about not understanding it)! It really evolved over that time from one thing into another. I believe that a significant portion of those w/POTS will have an autoimmune cause (and I believe that it is possible that some day POTS will be considered an autoimmune disease but I know the science is not quite there yet).
My treatments were high dose IVIG and Rituximab. We do not believe that ME/CFS is my diagnosis (even though it started out that way and every doctor I saw in 2013 and 2014 gave me a "CFS" diagnosis). But in my case, it all shifted into autoimmunity and the treatments that helped me were both autoimmune treatments. Until there is a bio-marker, no one will know for sure which is why I was so interested in the ICC listing "ion transport issues" since this played a big role in my personal case.
I want to understand the reasoning for not using a calcium channel blocker. This will take some time for me, as I tire quickly when using my brain to sort this stuff out.
In my case it is b/c I have an autoantibody blocking the calcium channels so I am not to use meds or anesthesias that further block them b/c they would make me worse and could be dangerous.
Marylib
Senior Member
- Messages
- 1,171
@Gingergrrl
Thanks for the explanation. Yeah, maybe all of us with POTS are in the automimmune state. Seems likely, but who knows? There are people who are diagnosed with ME/CFS who do not have POTS. For ages, I just had the usual orthostatic intolerance.
In terms of ME/CFS, maybe the jury is still out on that one. There is so much more research happening in the last couple of years. I am no longer zealous about one case definition over the other, but Fukuda was ridiculous, in my opinion.
It is the insurance companies that drive me nuts. People have to hide from American insurance companies and from British psychiatrists. Australia turning into the US, in terms of money and power in some ways. Good thing that the research in Melbourne finally landed some money. Not enough, but better than it was.
Fortunately, no one pays much attention to New Zealand so we have it pretty good here in terms of health care in general. We just have to keep Australia from taking over in terms of what used to be local businesses. It's ridiculous. We had a lousy govt. in power for far too long and now we have a horrible housing crisis and homelessness has really taken hold. Leave it to me to change any conversation to politics! Well, any Aussie or Kiwi will understand there has always been playful banter between the two countries. So I don't mean any offense.
I always wanted to try IVIG, but rituximab scared me. I guess all we know now is where we are now, if that makes any sense. I always think back to some study they did in 2015 or so about how the immune signatures of people diagnosed with ME/CFS change over time.
As far as the ICC and calcium channelopathies, the only thing I would know to do is search the references and try to connect the dots as to who was doing what research at any particular time. I mean, you could write to those doing research but those people barely have time to eat lunch. Any spare time would go to seeking funding, I would think.
Thanks for the explanation. Yeah, maybe all of us with POTS are in the automimmune state. Seems likely, but who knows? There are people who are diagnosed with ME/CFS who do not have POTS. For ages, I just had the usual orthostatic intolerance.
In terms of ME/CFS, maybe the jury is still out on that one. There is so much more research happening in the last couple of years. I am no longer zealous about one case definition over the other, but Fukuda was ridiculous, in my opinion.
It is the insurance companies that drive me nuts. People have to hide from American insurance companies and from British psychiatrists. Australia turning into the US, in terms of money and power in some ways. Good thing that the research in Melbourne finally landed some money. Not enough, but better than it was.
Fortunately, no one pays much attention to New Zealand so we have it pretty good here in terms of health care in general. We just have to keep Australia from taking over in terms of what used to be local businesses. It's ridiculous. We had a lousy govt. in power for far too long and now we have a horrible housing crisis and homelessness has really taken hold. Leave it to me to change any conversation to politics! Well, any Aussie or Kiwi will understand there has always been playful banter between the two countries. So I don't mean any offense.
I always wanted to try IVIG, but rituximab scared me. I guess all we know now is where we are now, if that makes any sense. I always think back to some study they did in 2015 or so about how the immune signatures of people diagnosed with ME/CFS change over time.
As far as the ICC and calcium channelopathies, the only thing I would know to do is search the references and try to connect the dots as to who was doing what research at any particular time. I mean, you could write to those doing research but those people barely have time to eat lunch. Any spare time would go to seeking funding, I would think.
Gingergrrl
Senior Member
- Messages
- 16,171
Thanks for the explanation. Yeah, maybe all of us with POTS are in the automimmune state. Seems likely, but who knows? There are people who are diagnosed with ME/CFS who do not have POTS. For ages, I just had the usual orthostatic intolerance.
My feeling at this point, based on a lot of the new research, is that POTS is going to turn out to be an Autoimmune Disease (or at least a HUGE sub-group of those with POTS will have "Autoimmune POTS" like I do per my doctors). I think that many with ME/CFS have co-morbid POTS but there also may be some with ME/CFS that have the symptoms of POTS as part of their ME/CFS vs. having two separate co-morbid illnesses.
I am no longer zealous about one case definition over the other, but Fukuda was ridiculous, in my opinion.
I have never been zealous re: the name of the illness or the criteria. I created this thread b/c I was literally stunned to learn that one of the criteria (ICC) listed "ion transport" issues in the criteria and wanted to learn more about how this came to be listed.
Fortunately, no one pays much attention to New Zealand so we have it pretty good here in terms of health care in general.
That is great

Leave it to me to change any conversation to politics!
I am the same way and have to really monitor what I write on PR so I do not get into politics
I always wanted to try IVIG, but rituximab scared me.
IVIG has many uses for both immune deficiency and autoimmunity (even in case where the exact illness mechanism is not known). Versus Rituximab is for B-cell driven autoimmunity (in addition to cancer). I did (and still do) Rituximab for autoimmunity and now get infusions twice per year for maintenance.
As far as the ICC and calcium channelopathies, the only thing I would know to do is search the references and try to connect the dots as to who was doing what research at any particular time.
This is exactly what I hope to do at some point when I have more time. I want to look at the references and connect the dots how channelopathies got listed as part of the ICC criteria.
pattismith
Senior Member
- Messages
- 3,990
... the autoantibody that I have is called VGCC for "voltage gated calcium channel". I know that there are also "ligand" channels which are not voltage gated but I cannot explain much beyond knowing those words (which is a bummer b/c I really want to understand this better some day) and am now gobsmacked that there could be a connection to ME/CFS after all (from the ICC criteria).
Ginger,
could you remind me what type of VGCC antibodies you had and if they were lack of function Ab?
Here what I read about muscle contraction in wiki:
"L-type calcium channels are also enriched in the t-tubules of striated muscle cells, i.e., skeletal and cardiac myofibers.
When these cells are depolarized, the L-type calcium channels open as in smooth muscle. In skeletal muscle, the actual opening of the channel, which is mechanically gated to a calcium-release channel (a.k.a. ryanodine receptor, or RYR) in the sarcoplasmic reticulum (SR), causes opening of the RYR.
(In cardiac muscle, opening of the L-type calcium channel permits influx of calcium into the cell. The calcium binds to the calcium release channels (RYRs) in the SR, opening them; this phenomenon is called "calcium-induced calcium release", or CICR.)
However the RYRs are opened, either through mechanical-gating (squeletal muscle) or CICR (heart), Ca2+ is released from the SR and is able to bind to troponin C on the actin filaments. The muscles then contract through the sliding filament mechanism, causing shortening of sarcomeres and muscle contraction. "
I'm still investigating muscle channels as I had extreme weakness reaction to Azithromycin (dose dependant), and I found modulation of my muscle calcium homeostasis was very important in my disease.
There is a new study showing that azithromycin is blocking L type VGCC so it could explain why many patients who have muscle weakness with calcium muscle homeostasis impairment have problems with this kind of antibiotics (and not only patients with Myastenia Gravis or Periodic paralysis that are already known to badly react)...
I remember that @duncan listed POTS as one of the typical symptoms of Periodic Paralysis (which is not autoimmune). It seemed that the PP doctor I'm in contact with was not really surprised to hear I have POTS/dysautonomia, and it seemed he counted it to PP. Indeed, if I eat more carbohydrates than usual (which worsens POTS) and if I then take potassium, it gets better. I can't say if people with PP get autoimmunity more often (and if those with POTS have autoimmunity), but I think, based on this information, there exists non-autoimmune POTS, too.My feeling at this point, based on a lot of the new research, is that POTS is going to turn out to be an Autoimmune Disease
Sadly, still only RYRs are mentioned when it's about sceletal muscle functioning. This is not the entire picture. There's a reason why there are other ion channels in each muscle cell - because every ion channel is needed for a correct functioning of (sceletal) muscles; every calcium ion channel present is part of the calcium signaling cascade. It's only that the function of RYR in sceletal muscles is better understood. E.g. it is only begun to understand the role of IP3Rs in this respect.In skeletal muscle, the actual opening of the channel, which is mechanically gated to a calcium-release channel (a.k.a. ryanodine receptor, or RYR) in the sarcoplasmic reticulum (SR), causes opening of the RYR.
The same holds for cardiac muscle cells; or neuronal cells; or...
In several papers I read that e.g. one calcium ion channel type is more prevalent in a cell line than another type, and they often concluded the other type is redundant or has no function. Sure. That's why it's there; that's how nature works. In later papers you then read about the discovery of the function of this other type...
Oh, thinking of it, what I found interesting in a paper that looked at the biochemistry in Sjögren's: They found a link to IP3R3 (one type of ligand-gated calcium channel), and exosomes are mentioned as a "transporter" for miRNA in Fig. 7:
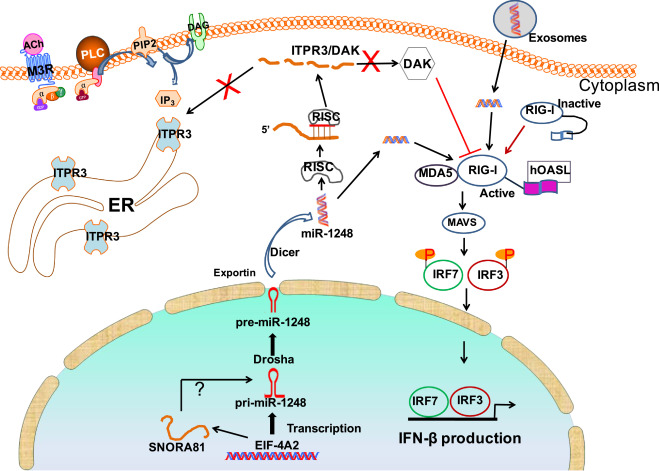
https://www.sciencedirect.com/science/article/pii/S2352396419306085
So exosomes are connected to signaling? Having the exosome findings in ME in mind, does that point to a signaling disruption? Also, I remember there was a paper about elevated miRNA in ME (I think by Scheibenbogen et al.?) - if exosomes transport miRNA, are both findings connected? One group found the exosomes (but not the miRNA they carried), the other the miRNA (but not the exosomes)?
pattismith
Senior Member
- Messages
- 3,990
@Inara
about muscle IP3 receptor role, In this study, it is well explained:
"Tetanic electrical stimulation induces two separate calcium signals in rat skeletal myotubes,
-a fast one, dependent on Cav 1.1 or dihydropyridine receptors (DHPRs) and ryanodine receptors and related to contraction,
-and a slow signal, dependent on DHPR and inositol trisphosphate receptors (IP3Rs) and related to transcriptional events.
......
The slow Ca2+ signal has a role in transcription activation of several genes in cultured myotubes ...
......
We can speculate that in adult muscle, slow Ca2+ signals act as a decoding tool of different stimulation patterns incoming from the motor neuron, which participate in muscle plasticity.
The fact that slow Ca2+ signals were not present in slow muscle fibers and the fact that they participate in regulation of slow-type genes in fast fibers would suggest that the slow Ca2+ signal is involved in the induction of a slow phenotype, mediated by a particular pattern of electrical stimulation of fast muscle fibers."
about muscle IP3 receptor role, In this study, it is well explained:
"Tetanic electrical stimulation induces two separate calcium signals in rat skeletal myotubes,
-a fast one, dependent on Cav 1.1 or dihydropyridine receptors (DHPRs) and ryanodine receptors and related to contraction,
-and a slow signal, dependent on DHPR and inositol trisphosphate receptors (IP3Rs) and related to transcriptional events.
......
The slow Ca2+ signal has a role in transcription activation of several genes in cultured myotubes ...
......
We can speculate that in adult muscle, slow Ca2+ signals act as a decoding tool of different stimulation patterns incoming from the motor neuron, which participate in muscle plasticity.
The fact that slow Ca2+ signals were not present in slow muscle fibers and the fact that they participate in regulation of slow-type genes in fast fibers would suggest that the slow Ca2+ signal is involved in the induction of a slow phenotype, mediated by a particular pattern of electrical stimulation of fast muscle fibers."
@pattismith, thank you! Yes, I remember the paper now.
pattismith
Senior Member
- Messages
- 3,990
@pattismith, thank you! Yes, I remember the paper now.
The calcium signaling is such a complex thing to understand!
About miRNA, it can be involved in diseases, but I don't know if miRNA produced in myocytes can damage other tissu cells.
On the other hand, circRNA is another noncoding RNA that can be found into exosomes. circRNA inhibits gene modulation of miRNA, and circRNA have shown to potentially damage tissus far from their production site.
Last edited:
Marylib
Senior Member
- Messages
- 1,171
@pattismith That is really interesting - I wish I fully understood it. When you say you found the part about muscle contraction in wiki, do you have a link to have a link to that? There are so many various wiki's floating around these days. Thanks. No rush. I have been trying to understand what type of heart failure that the calcium channel blockers are designed to treat. The only thing I know is that you need to have your kidney function tested if you take a calcium channel blocker.Ginger,
could you remind me what type of VGCC antibodies you had and if they were lack of function Ab?
Here what I read about muscle contraction in wiki:
"L-type calcium channels are also enriched in the t-tubules of striated muscle cells, i.e., skeletal and cardiac myofibers.
When these cells are depolarized, the L-type calcium channels open as in smooth muscle. In skeletal muscle, the actual opening of the channel, which is mechanically gated to a calcium-release channel (a.k.a. ryanodine receptor, or RYR) in the sarcoplasmic reticulum (SR), causes opening of the RYR.
(In cardiac muscle, opening of the L-type calcium channel permits influx of calcium into the cell. The calcium binds to the calcium release channels (RYRs) in the SR, opening them; this phenomenon is called "calcium-induced calcium release", or CICR.)
However the RYRs are opened, either through mechanical-gating (squeletal muscle) or CICR (heart), Ca2+ is released from the SR and is able to bind to troponin C on the actin filaments. The muscles then contract through the sliding filament mechanism, causing shortening of sarcomeres and muscle contraction. "
I'm still investigating muscle channels as I had extreme weakness reaction to Azithromycin (dose dependant), and I found modulation of my muscle calcium homeostasis was very important in my disease.
There is a new study showing that azithromycin is blocking L type VGCC so it could explain why many patients who have muscle weakness with calcium muscle homeostasis impairment have problems with this kind of antibiotics (and not only patients with Myastenia Gravis or Periodic paralysis that are already known to badly react)...
pattismith
Senior Member
- Messages
- 3,990
https://en.wikipedia.org/wiki/Voltage-gated_calcium_channel@pattismith That is really interesting - I wish I fully understood it. When you say you found the part about muscle contraction in wiki, do you have a link to have a link to that? There are so many various wiki's floating around these days. Thanks. No rush. I have been trying to understand what type of heart failure that the calcium channel blockers are designed to treat. The only thing I know is that you need to have your kidney function tested if you take a calcium channel blocker.
pattismith
Senior Member
- Messages
- 3,990
@Inara
I read some interesting stuff about IP3, maybe you are interested:
IP3R deficit underlies loss of salivary fluid secretion in Sjögren’s Syndrome
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047094/
and
Mice Lacking Inositol 1,4,5-Trisphosphate Receptors Exhibit Dry Eye
scientific community got interested in inhibitory antibodies against muscarinic receptors M3 in Sjogren syndrome:
"M3 muscarinic acetylcholine receptor (M3R) plays a crucial role in the secretion of saliva from salivary glands. It is reported that some patients with Sjögren's syndrome (SS) carried inhibitory autoantibodies against M3R."
and M3R activation is mediated by IP3R...
I read some interesting stuff about IP3, maybe you are interested:
IP3R deficit underlies loss of salivary fluid secretion in Sjögren’s Syndrome
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047094/
and
Mice Lacking Inositol 1,4,5-Trisphosphate Receptors Exhibit Dry Eye
scientific community got interested in inhibitory antibodies against muscarinic receptors M3 in Sjogren syndrome:
"M3 muscarinic acetylcholine receptor (M3R) plays a crucial role in the secretion of saliva from salivary glands. It is reported that some patients with Sjögren's syndrome (SS) carried inhibitory autoantibodies against M3R."
and M3R activation is mediated by IP3R...
Yes, thanks @pattismith!
The one I linked above,
https://www.sciencedirect.com/science/article/pii/S2352396419306085,
is also about the role of IP3Rs in Sjögren's.
It seems to me the calcium signaling topic is gaining more and more interest, maybe?
The one I linked above,
https://www.sciencedirect.com/science/article/pii/S2352396419306085,
is also about the role of IP3Rs in Sjögren's.
It seems to me the calcium signaling topic is gaining more and more interest, maybe?
Gingergrrl
Senior Member
- Messages
- 16,171
It seems to me the calcium signaling topic is gaining more and more interest, maybe?
I think it is gaining more interest (or at least I hope it is
) and I am planning to read all of the new posts in this thread in more detail before I reply. I wish I could understand everything that was posted Gingergrrl
Senior Member
- Messages
- 16,171
I just got a chance to read through the newer posts and want to reply to a few things...
I have the N-type Calcium Channel Autoantibody. It was first discovered that I had it on the Mayo Panel called "PAVAL" in early 2016 and re-confirmed that I still have it on the Mayo Panel called "DYS1" in 2018.
What do you mean by "lack of function Ab"? Sorry I don't understand
My understanding is that there is no commercial test for the L-type calcium channel autoantibody outside of research studies. The panels that I did tested only the N-type (which I have) and the P/Q type (which I do not have). I really would love to be tested for the L-type b/c Propofol (anesthesia) is an L-type calcium channel blocker and I want to know if it would be unsafe for me to have it (if I should ever need it in the future).
That is very interesting and there are warnings now (in the US, not sure if world-wide) that Azithromycin (often called Z-pack here) can cause cardiac problems. It is another one that I 100% avoid. What did you mean that you found calcium homeostasis very important in your disease? How did you know what to do when you had the reaction to Azithromycin?
There are also black box warnings for Fluoroquinolone antibiotics that people with myasthenia gravis should NOT take them. I had a neurotoxic reaction to Levaquin (an FQ antibiotic) in 2010 which started my entire illness. It caused systemic weakness and cardiac issues and severely injured my right triceps tendon. I was in excellent health prior to taking Levaquin. But two yrs later I got severe mono from EBV following a minor surgery and then about ten months after that, we moved into a rental w/toxic black mold. So I had three immune triggers back to back and can never know for sure at this point what caused what.
I remember and I think I told you that almost every single person in my FB group who has the N-type CA+ Channel autoantibody also has POTS. Although in that case, they do have autoimmunity with the CA+ Channel Ab.
I totally agree with you but am not sure if there are illnesses in which POTS is a symptom of that illness vs. POTS also being an illness in and of itself. It makes me wonder if POTS (as a stand-alone illness) is autoimmune vs. having POTS as part of another illness may not be? But I am just guessing and really have no clue!
Can you remind me what "RYR" means?
Me, too
My understanding is that calcium channel blockers prevent or block calcium from going into the cells of the heart (or the blood vessels?) in people in which there is already calcium build-up or a blockage? In my case, calcium is already being blocked from going into the cells by the autoantibody so I am not supposed to take any meds that further block this from happening. Hopefully someone more sciency than me (which is just about everyone) can explain this better
Ginger, could you remind me what type of VGCC antibodies you had and if they were lack of function Ab?
I have the N-type Calcium Channel Autoantibody. It was first discovered that I had it on the Mayo Panel called "PAVAL" in early 2016 and re-confirmed that I still have it on the Mayo Panel called "DYS1" in 2018.
What do you mean by "lack of function Ab"? Sorry I don't understand
Here what I read about muscle contraction in wiki:
"L-type calcium channels are also enriched in the t-tubules of striated muscle cells, i.e., skeletal and cardiac myofibers.
My understanding is that there is no commercial test for the L-type calcium channel autoantibody outside of research studies. The panels that I did tested only the N-type (which I have) and the P/Q type (which I do not have). I really would love to be tested for the L-type b/c Propofol (anesthesia) is an L-type calcium channel blocker and I want to know if it would be unsafe for me to have it (if I should ever need it in the future).
I'm still investigating muscle channels as I had extreme weakness reaction to Azithromycin (dose dependant), and I found modulation of my muscle calcium homeostasis was very important in my disease.
That is very interesting and there are warnings now (in the US, not sure if world-wide) that Azithromycin (often called Z-pack here) can cause cardiac problems. It is another one that I 100% avoid. What did you mean that you found calcium homeostasis very important in your disease? How did you know what to do when you had the reaction to Azithromycin?
There is a new study showing that azithromycin is blocking L type VGCC so it could explain why many patients who have muscle weakness with calcium muscle homeostasis impairment have problems with this kind of antibiotics (and not only patients with Myastenia Gravis or Periodic paralysis that are already known to badly react)...
There are also black box warnings for Fluoroquinolone antibiotics that people with myasthenia gravis should NOT take them. I had a neurotoxic reaction to Levaquin (an FQ antibiotic) in 2010 which started my entire illness. It caused systemic weakness and cardiac issues and severely injured my right triceps tendon. I was in excellent health prior to taking Levaquin. But two yrs later I got severe mono from EBV following a minor surgery and then about ten months after that, we moved into a rental w/toxic black mold. So I had three immune triggers back to back and can never know for sure at this point what caused what.
I remember that @duncan listed POTS as one of the typical symptoms of Periodic Paralysis (which is not autoimmune).
I remember and I think I told you that almost every single person in my FB group who has the N-type CA+ Channel autoantibody also has POTS. Although in that case, they do have autoimmunity with the CA+ Channel Ab.
but I think, based on this information, there exists non-autoimmune POTS, too.
I totally agree with you but am not sure if there are illnesses in which POTS is a symptom of that illness vs. POTS also being an illness in and of itself. It makes me wonder if POTS (as a stand-alone illness) is autoimmune vs. having POTS as part of another illness may not be? But I am just guessing and really have no clue!
Sadly, still only RYRs are mentioned when it's about sceletal muscle functioning.
Can you remind me what "RYR" means?
@pattismith That is really interesting - I wish I fully understood it.
Me, too
I have been trying to understand what type of heart failure that the calcium channel blockers are designed to treat.
My understanding is that calcium channel blockers prevent or block calcium from going into the cells of the heart (or the blood vessels?) in people in which there is already calcium build-up or a blockage? In my case, calcium is already being blocked from going into the cells by the autoantibody so I am not supposed to take any meds that further block this from happening. Hopefully someone more sciency than me (which is just about everyone) can explain this better
Marylib
Senior Member
- Messages
- 1,171
@Gingergrrl I guess that kinda makes sense about the calcium being diverted from the blood vessels. Maybe it is like some kind of switch that moves calcium around. I have no idea!
Has it already been posted?
https://www.sciencedirect.com/science/article/pii/S2213158219303924#bib0032
"The role of Ca2+ in relevant astrocyte support and/or oscillatory performance of RAS neurons is yet to be established. It is also worth noting that neuroinflammation has been observed in ME/CFS (Nakatomi et al., 2014) and that the brainstem is particularly sensitive to hypoxia (Marina et al., 2015). While the consequences of RAS connectivity deficits in such a complex system are difficult to predict, they can be expected to influence initiation and maintenance of movement, sleep quality, autonomic function and cortical arousal levels which affect memory, learning and problem solving, and therefore contribute to many of the symptoms of ME/CFS."
https://www.sciencedirect.com/science/article/pii/S2213158219303924#bib0032
"The role of Ca2+ in relevant astrocyte support and/or oscillatory performance of RAS neurons is yet to be established. It is also worth noting that neuroinflammation has been observed in ME/CFS (Nakatomi et al., 2014) and that the brainstem is particularly sensitive to hypoxia (Marina et al., 2015). While the consequences of RAS connectivity deficits in such a complex system are difficult to predict, they can be expected to influence initiation and maintenance of movement, sleep quality, autonomic function and cortical arousal levels which affect memory, learning and problem solving, and therefore contribute to many of the symptoms of ME/CFS."