Yasko also believes that the bottleneck is low levels of Bh4
Agreed, and she deserves credit for fishing out that connection. However she believes BH4 is depleted because increased ammonia makes NOS run backwards and somehow that when it runs backwards it uses up BH4.
There are two things wrong with this. First, NOS is/are the enzyme(s) that produce NO. It doesn't come from anywhere else that I know of. The equation is:
2 L-arginine + 3 NADPH + 1 H+ + 4 O2  2 citrulline +2 nitric oxide + 4 H2O + 3 NADP+
2 citrulline +2 nitric oxide + 4 H2O + 3 NADP+
Basically arginine is transformed into citruline + NO. Yasko argues that when we have extra ammonia it can cause NOS to run "backwards," taking citrulline and NO and creating arginine. But to have NO NOS has to run forwards in order to produce it. So there's no net change in the amount of citrulline from NOS. Even assuming high citrulline (and
Naviaux found serum citrulline to be normal for us) it would mostly result in NOS inactivity as levels of arginine, citrulline, and nitric oxide reached an equilibrium. I don't see it resulting in a bunch of arginine production. Yasko's theory hinges partly on high citrulline causing high arginine synthesis via NOS, which appears to me impossible.
The second problem with Yasko's theory regarding NOS is that when NOS runs backwards it uses up BH4. BH4 is a cofactor for NOS but it is not "used up" by it (See
Wikipedia: "Tetrahydrobiopterin provides an additional electron during the catalytic cycle which is replaced during turnover.") At best some of the NO that NOS produces will combine with superoxide to form peroxynitrite, which oxidizes BH4. This explanation wouldn't work, however, if NOS was somehow--magically perhaps--producing net movement towards arginine by using up citrulline and NO.
But Yasko isn't just wrong about how NOS effects BH4, she's wrong about how MTHFR effects BH4: She suggests that MTHFR runs "backwards" to convert BH2 (q-BH2 actually) to BH4, which
has only been shown in vitro when you add very high concentrations of 5-MTHF--concentrations would almost certainly cause "methyltrap." Methyltrap is a condition where 5-MTHF cannot be converted because there is no B12 for methionine synthase, and MTHFR normally doesn't run backwards, thus methylfolate is "trapped." So even if we could reach the necessary concentrations of 5-MTHF to run MTHFR backwards, we would also create a "methyltrap," which is quite uncomfortable and unhealthy.
In summary, Yasko may be getting parts of treatment right but I think she's getting decent chunks of theory dead-wrong.
Why is it that you think that the nadph is the reason malic helps over the malate to Aspartate conversion? Being that we are hypometabolic specifically in Tca cycle it makes sense we'd be putting out a low level of Aspartate.
This is where Yasko's bad theories can lead to some bad or ineffective treatments, I believe.
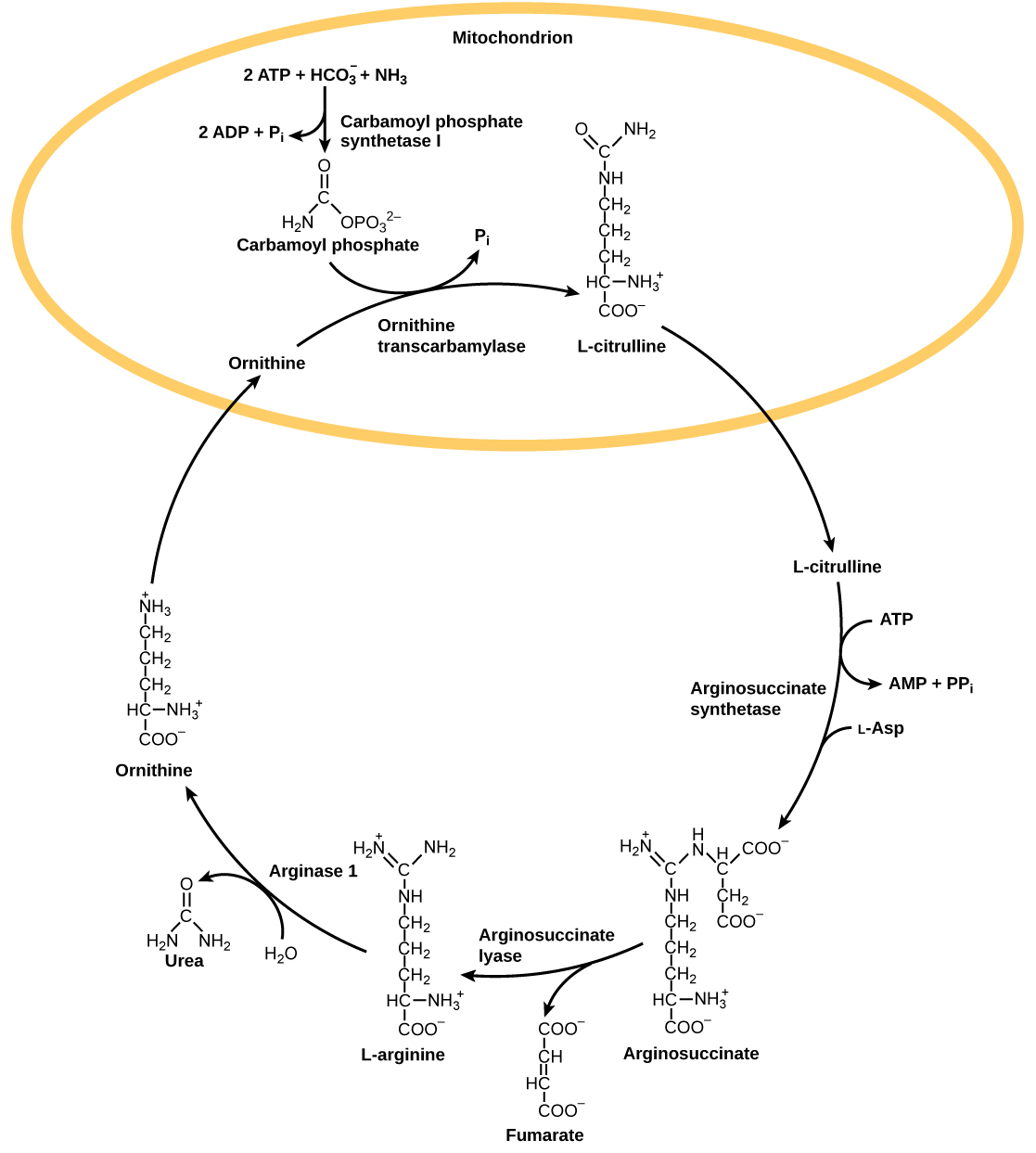
Under Yasko's theory the problem is 1. That we make too much ammonia and possibly 2. That because of krebs cycle problems we might have uric acid cycle blocks that forces ammonia to use the NOS "shortcut." The second point was my original reasoning behind why malic acid helped me. But if we truly didn't have enough aspartate to combine with citrulline to form argininosuccinate then we should have high citrulline--and as I pointed out above, Naviaux didn't find this. Maybe we have low aspartate, maybe we have low malate, maybe supplementing malic acid or aspartate helps fill holes in our biochemisty and we feel better for that, but as far as I can tell aspartate isn't low
enough to impact the urea cycle.
One final note: I have concerns with using Citrulline and Arginine as supplements. Even if one buys into Yasko's view of things, L-Citrulline would seem to be a bad choice, as it is essentially an ammonia carrier. And even if one were trying to unblock the urea cycle in order to move more ammonia through it, adding a molecule already carrying ammonia seems like a poor choice.
Arginine, like citrulline, is essentially carrying ammonia. Unlike citrulline, it is an amino acid used to make proteins and nitric oxide. Scientists have studied arginine as a possible way to prevent heart attacks. And there were some positive indications. But then
this study which gave arginine to patients starting after their first heart attack was ended early when six patients in the treatment group died (none of the control group did). It may be that the difference had something to do with higher production of asymmetric dimethyl arginine from arginine; that since high ADMA:arginine is a risk factor for heart disease many heart attack patients have an already high ratio of ADMA:arginine, and adding more arginine only ends up producing more ADMA for them.
In any case, Naviaux found high serum arginine, so I'm not sure why we would want to supplement more.
Ornithine (and here I'm just reading off the
biochemical pathways map, so I'm not sure how prevalent this is) can be converted to glutamate, and glutamate is what the body uses to transport ammonia. So if ammonia is really the problem, then excess ornithine is potentially a problem too.