

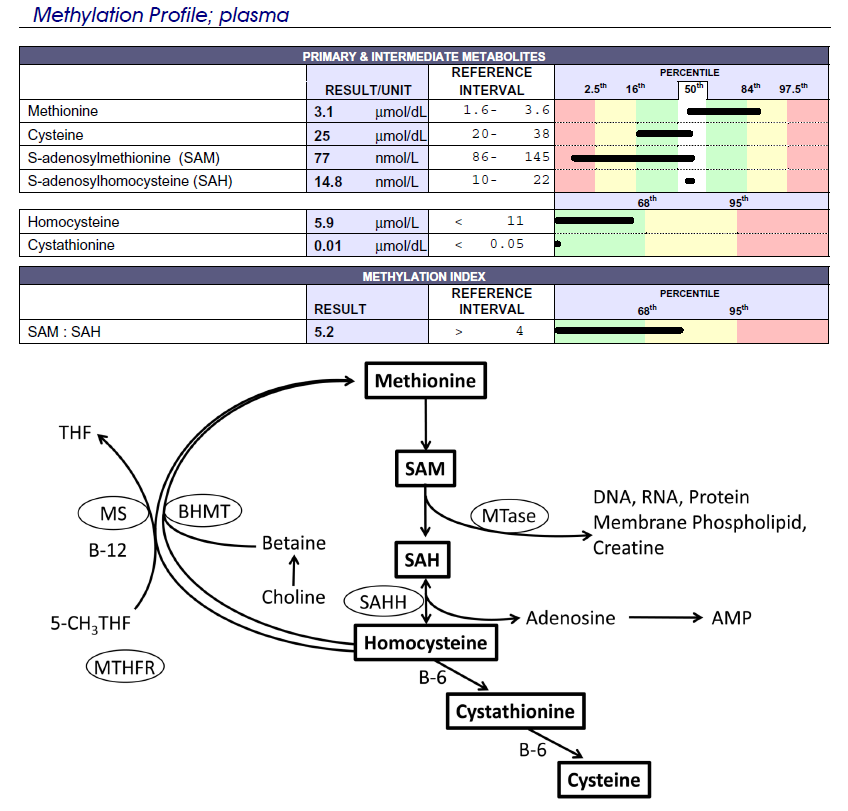
Seems like there's a block going from Met -> SAM.
I found this thread which had a lot of good info by @DREBS
http://forums.phoenixrising.me/inde...thionine-yet-blocked-methylation-cycle.23785/
Apparently ATP and magnesium are the cofactors for Met -> SAM. I take loads of magnesium glycinate, it helps all my symptoms and helps my sleep so I don't think that's the problem.
I did Genova's Nutreval and my krebs wasn't in great shape, so that might corroborate a low ATP hypothesis.
http://imgur.com/pQLGBw2
http://imgur.com/uJmmBK6
Genova has an awesome interpretation guide for that and I've been following its suggestions.
https://www.gdx.net/core/interpretive-guides/Organix-IG.pdf
Does anyone have any other ideas, as to what might be the problem here?
I found this thread which had a lot of good info by @DREBS
http://forums.phoenixrising.me/inde...thionine-yet-blocked-methylation-cycle.23785/
Apparently ATP and magnesium are the cofactors for Met -> SAM. I take loads of magnesium glycinate, it helps all my symptoms and helps my sleep so I don't think that's the problem.
I did Genova's Nutreval and my krebs wasn't in great shape, so that might corroborate a low ATP hypothesis.
http://imgur.com/pQLGBw2
http://imgur.com/uJmmBK6
Genova has an awesome interpretation guide for that and I've been following its suggestions.
https://www.gdx.net/core/interpretive-guides/Organix-IG.pdf
Does anyone have any other ideas, as to what might be the problem here?
") ... but I didn't continue since it is super expensive.
... but I didn't continue since it is super expensive.