Joey,
many thanks for your reply. I always learn a lot from your posts.
Hey Garcia,
Genova told me that ++ = BB, meaning B is the mutation. If true this would go against the grain of genotyping nomenclature, which is odd to say the least.
You/they are right. Thanks for correcting me. It does appear that BB is the mutation for Bsm.
I don't know if it is the same case with Yasko's test, but I hope not because most of the results I'm hearing on the Yasko test are ++, meaning most of us have the worst genotype for gcmaf (as far as Bsm is concerned). This includes myself.
However, I think none of us should rely on Yasko's testing to make such an important decision. I simply don't trust Yasko's lab... the fact that they offered Bsm and Taq as one result and told me that it's because they're usually same just increased my suspicions about their pseudoscientific genomic testing.
I've looked into this issue today and from my (admittedly limited investigations) it does appear that what Yasko is saying may be correct. Taq and Bsm do seem to correlate with one another. In the earlier tests it seems Yasko used to test all 3 VDR genes (Fok, Taq & Bsm), but she stopped testing Bsm (my test doesn't have a Bsm result), because the Bsm result most-often follows the Taq result. In this way Yasko was able to offer another snp test for the same price.
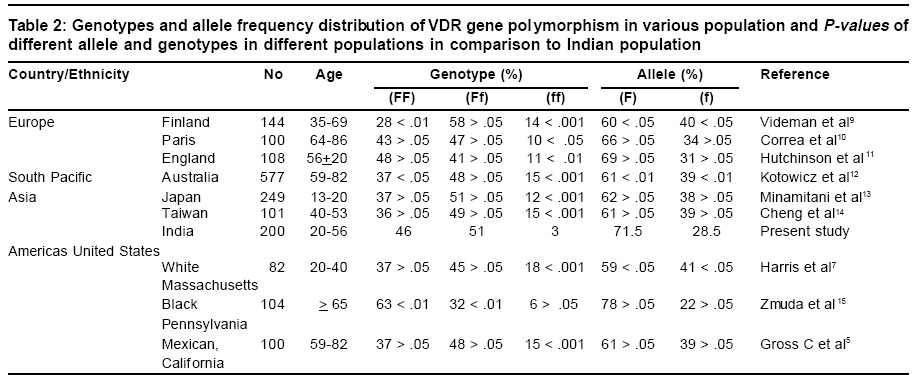
I've been looking at a few VDR studies online on population distributions of Taq & Bsm, and the numbers do seem to correlate (i.e. the numbers of tt would roughly equal BB, Tt would roughly equal Bb and TT would equal bb). Ok the numbers alone don't tell us if the exact same people who have tt have BB etc. (we need joint distributions for that), but then I also found this study here:
http://www.springerlink.com/content/9hjra4g5wxd814tc/
which looks at 3 VDR snps: Apa, Bsm, and Taq. In particular they say:
The most common genotypes observed in our population were AaBbTt (37%), AABBtt (20%), aabbTT (15%), AabbTT (15%), and AABbTt (9%).
Ignore the Aa part since we are not interested in the Apa snp. But as you can see all of the above groups are people for whom Bsm and Taq are correlated (i.e. if BB then tt, if bb then TT, if Bb then Tt). Together that accounts for (37+20+15+15+9 =) 95% of the population. i.e. in that group of 120 people 95% had Bsm and Taq correlated.
So it does seem that what Yasko is saying is true.
If you have an old-style Yasko test, then Bsm value is directly given. If it is -- then as Joey said you are BB which is the desired group.
If you have a new-style Yasko test like I do, then there is no Bsm listed. However the chances are your Bsm will correlate with your Taq (which is listed).
For example my Taq is ++ or tt, so there is a high (95%???) chance that I am Bsm BB unfortunately.
To find out for sure I'm going to post off my test to redlabs.
I hope all that hasn't confused anyone too much!
garcia.


") victory
victory