Most resources about Ehlers-Danlos syndrome emphasize the joint hypermobility and/or skin elasticity aspects without making it clear whether it's possible to have it without these “textbook symptoms”. Despite being familiar with EDS for years, I just kept brushing it aside until recently because those features didn't apply to me. What led me to suspect is the variety of morphological deformities I present with such as scoliosis, pectus excavatum, overbite, peyronie's disease, etc. These are strongly indicative of a connective tissue disorder. In addition, I have many of the common comorbidities such as dysautonomia, strongly suspected MCAS, severe digestive problems, etc. amounting to at least 75% of the problems listed on this page: http://ohtwist.com/about-eds/comorbidities/
Since I am not hypermobile (on the contrary, my body is quite stiff and achy), I didn't pass the Beighton test. My rheumatologist then referred me to a geneticist for evaluation on EDS and Marfan's, who unfortunately won't see me until March. I know that at least part of this genetically rooted. My mother was diagnosed with CFS, POTS, Sjogren's and MCAS and shares many of my symptoms. My maternal grandmother contracted a 'flu that never went away' in her 40s. A difference between me and them is their lack of the morphological problems that I have. I think it's because of my onset happening during infancy, meaning my skeletal system formed post-trigger, after the deadly reaction to antibiotics, whereas both my mother and grandmother were debilitated during middle age. I understand that a relatively normal period of life followed by a “trigger” of some sort, usually injury, infection or chemical exposure, is a common pattern in this spectrum of illnesses. The only other common markers of EDS I can think of – my joints often crack with movement and I always discover scratches and bruises of unknown origin on my skin, but I never thought much of it.
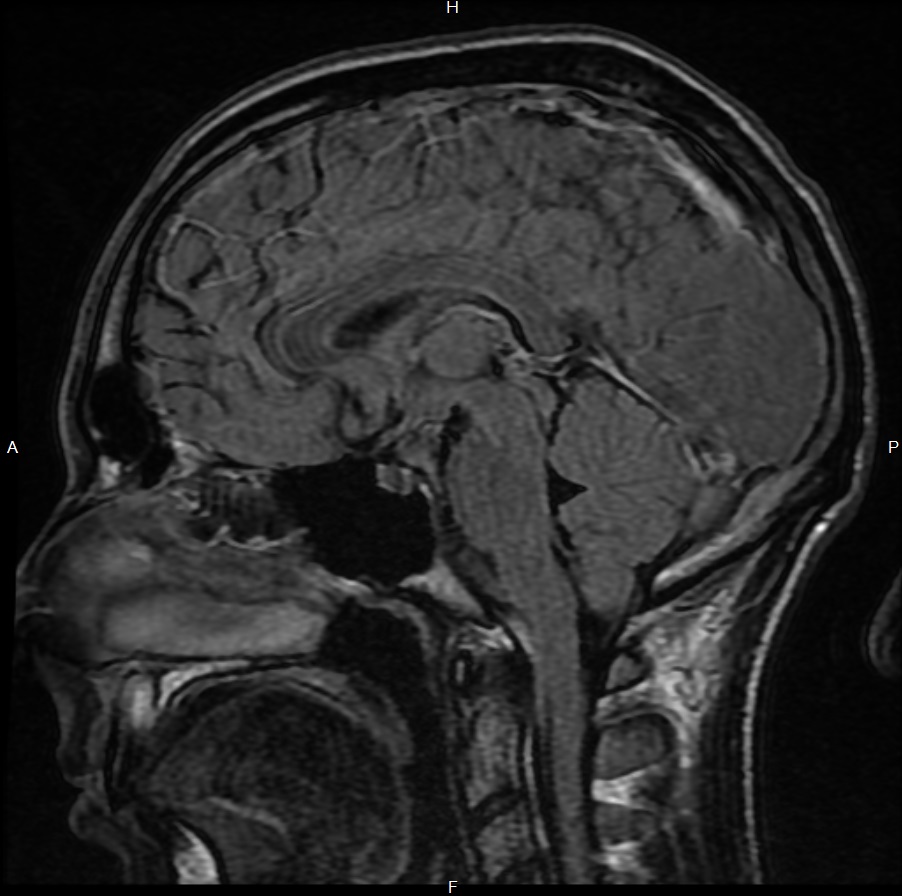
One of my worst lifelong symptoms is the severe headache that I have radiating from the base of my skull to my head, neck, and trapezius regions. It's a very nasty pain accompanied by a feeling of pressure as if I'm deep underwater and ringing in my ears. The pain worsens with standing , swallowing, bending down, etc. Chiari malformation would explain this pain with such precision, but my brain and neck MRIs were interpreted as being normal.
It's also worth noting that some specialists are classifying MCAS as a variety of EDS...
Since I am not hypermobile (on the contrary, my body is quite stiff and achy), I didn't pass the Beighton test. My rheumatologist then referred me to a geneticist for evaluation on EDS and Marfan's, who unfortunately won't see me until March. I know that at least part of this genetically rooted. My mother was diagnosed with CFS, POTS, Sjogren's and MCAS and shares many of my symptoms. My maternal grandmother contracted a 'flu that never went away' in her 40s. A difference between me and them is their lack of the morphological problems that I have. I think it's because of my onset happening during infancy, meaning my skeletal system formed post-trigger, after the deadly reaction to antibiotics, whereas both my mother and grandmother were debilitated during middle age. I understand that a relatively normal period of life followed by a “trigger” of some sort, usually injury, infection or chemical exposure, is a common pattern in this spectrum of illnesses. The only other common markers of EDS I can think of – my joints often crack with movement and I always discover scratches and bruises of unknown origin on my skin, but I never thought much of it.
One of my worst lifelong symptoms is the severe headache that I have radiating from the base of my skull to my head, neck, and trapezius regions. It's a very nasty pain accompanied by a feeling of pressure as if I'm deep underwater and ringing in my ears. The pain worsens with standing , swallowing, bending down, etc. Chiari malformation would explain this pain with such precision, but my brain and neck MRIs were interpreted as being normal.
It's also worth noting that some specialists are classifying MCAS as a variety of EDS...