At Suzy's suggestion, Cort added the COalition 4 ME/CFS response to the DSM-5 into this thread as well as the coalition call to action here.
I think the link to the response that the Coalition submitted might have been lost in the process - at least from what I can tell. Here's a high level summary and links to both the coalition position paper and the coalition response.
1. High level summary of the issues
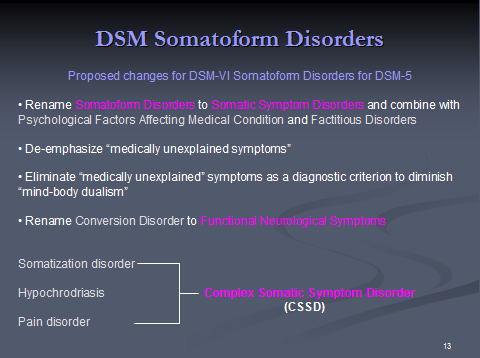
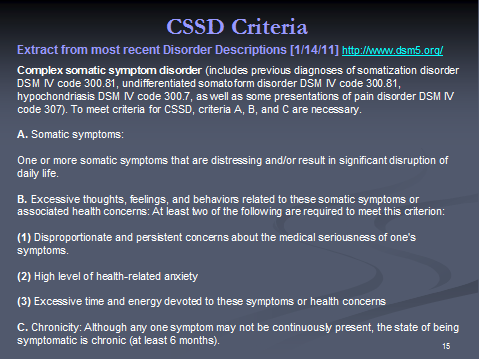
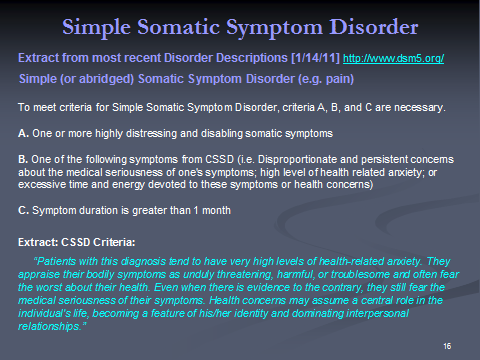
Among other changes, the DSM-5 proposal includes the establishment of a new category called Complex Somatic Symptom Disorder (CSSD). The criteria for a CSSD diagnosis include somatic symptoms that last more than 6 months and significantly disrupt life combined with the doctors assessment that the patient has a disproportionate concern about the medical seriousness of his symptoms. The guidelines also include recommendations of Cognitive Behavior Therapy (CBT) and antidepressants as the appropriate therapies.
CSSD could prove disastrous for the ME/CFS patient and for patients with other diseases like Fibromyalgia, Gulf War Illness and IBS that are misunderstood, misdiagnosed and mistreated by the medical community at large. For doctors who view the ME/CFS patient as just depressed, it will be a small leap to decide that the patient has disproportionate and persistent concerns about the medical seriousness of one's symptoms and, as a result, inappropriately diagnose CSSD. Once diagnosed with CSSD, the implications for diagnosis, treatment, disability and insurance will be profound.
2. The DSM-5 position paper with further details on the issue and the process to submit comments. This is based on the DSM-5 proposal as it exists this year (May, 2011)
3. The response that was submitted to the DSM-5 teamhttp://www.coalition4mecfs.org/DSM5letter.html by the Coalition 4 ME/CFS.
As Suzy said, each person or organization needs to submit their own comments on the web site using this process. You can either use the above materials to compose your own letter or use the letter directly.
I think the link to the response that the Coalition submitted might have been lost in the process - at least from what I can tell. Here's a high level summary and links to both the coalition position paper and the coalition response.
1. High level summary of the issues
Among other changes, the DSM-5 proposal includes the establishment of a new category called Complex Somatic Symptom Disorder (CSSD). The criteria for a CSSD diagnosis include somatic symptoms that last more than 6 months and significantly disrupt life combined with the doctors assessment that the patient has a disproportionate concern about the medical seriousness of his symptoms. The guidelines also include recommendations of Cognitive Behavior Therapy (CBT) and antidepressants as the appropriate therapies.
CSSD could prove disastrous for the ME/CFS patient and for patients with other diseases like Fibromyalgia, Gulf War Illness and IBS that are misunderstood, misdiagnosed and mistreated by the medical community at large. For doctors who view the ME/CFS patient as just depressed, it will be a small leap to decide that the patient has disproportionate and persistent concerns about the medical seriousness of one's symptoms and, as a result, inappropriately diagnose CSSD. Once diagnosed with CSSD, the implications for diagnosis, treatment, disability and insurance will be profound.
2. The DSM-5 position paper with further details on the issue and the process to submit comments. This is based on the DSM-5 proposal as it exists this year (May, 2011)
3. The response that was submitted to the DSM-5 teamhttp://www.coalition4mecfs.org/DSM5letter.html by the Coalition 4 ME/CFS.
As Suzy said, each person or organization needs to submit their own comments on the web site using this process. You can either use the above materials to compose your own letter or use the letter directly.