Dx Revision Watch
Suzy Chapman Owner of Dx Revision Watch
- Messages
- 3,061
- Location
- UK
ALERT: DSM-5 second public review period now running from May to 15 June
May be reposted in full or in part if source credited
I am resurrecting the existing DSM-5 thread in order that extensive previous material and comment is not lost. There was also discussion of DSM-5 on a second thread, here:
http://forums.phoenixrising.me/showthread.php?3062-DSM5-Ticket-back-to-Reevesville/page17
Please note that for a number of reasons, I no longer participate in these forums and I will not be monitoring this thread and won't be available to discuss the DSM-5 issue but I did feel that readers should be alerted to the following:
ALERT: The second Public Review of draft proposals for criteria and structure for DSM-5 is now open and runs from May to 15th June
This information was posted on Co-Cure mailing list, yesterday:
http://listserv.nodak.edu/cgi-bin/wa.exe?A2=ind1105a&L=co-cure&T=0&F&S&P=2584
Two attachments provided at foot of post.
Yesterday, 4 May, the American Psychiatric Association (APA) announced that a second public review period will run from May to 15 June. This is a revision of its Timeline, as it had stood in March, which had scheduled a public review exercise for August to 30 September.
There has been some media coverage of the APA's announcement here:
http://www.medpagetoday.com/Psychiatry/DSM-5/26275
http://thechart.blogs.cnn.com/2011/05/04/psychiatry-bible-structure-overhauled/
The DSM-5 site was updated yesterday with announcements and revised proposals (dated May 4, 2011) across all categories.
The current review period closes on 15th June - just six weeks away.
Note that this is a public and stakeholder review and feedback exercise and not restricted to professionals or members of the American Psychiatric Association.
There is a Task Force announcement here:
http://www.dsm5.org/Pages/Default.aspx
"What Specifically Has Changed on This Site?
"You will notice several changes to this Web site since we first launched in February 2010. Numerous disorders contain updated criteria...
"...Is There Opportunity to Provide Further Comments?
"At this time, we are asking visitors to review and comment on the proposed DSM-5 organizational structure and criteria changes. Please note that the current commenting period will end on June 15, 2011. It is important to remember that the proposed structure featured here is only a draft. These proposed headings were reviewed by the DSM-5 Task Force in November 2010...
"...The content on this site will stay in its current form until after completion of the DSM-5 Field Trials, scheduled to conclude later this year. Following analysis of field trial results, we will revise the proposed criteria as needed and, after appropriate review and approval, we will post these changes on this Web site. At that time, we will again open the site to a third round of comments from visitors, which will be systematically reviewed by each of the work groups for consideration of additional changes. Thus, the current commenting period is not the final opportunity for you to submit feedback, and subsequent revisions to DSM-5 proposals will be jointly informed by field trial findings as well as public commentary.
"We look forward to receiving your feedback during the coming weeks and appreciate your participation in this important process."
There are brief notes on the proposed DSM-5 Organizational Structure here:
http://www.dsm5.org/proposedrevision/Pages/proposed-dsm5-organizational-structure.aspx
The Recent updates page is here:
http://www.dsm5.org/Pages/RecentUpdates.aspx
The latest revisions for "Somatic Symptom Disorders" are here:
http://www.dsm5.org/ProposedRevision/Pages/SomaticSymptomDisorders.aspx
"Somatic Symptom Disorders
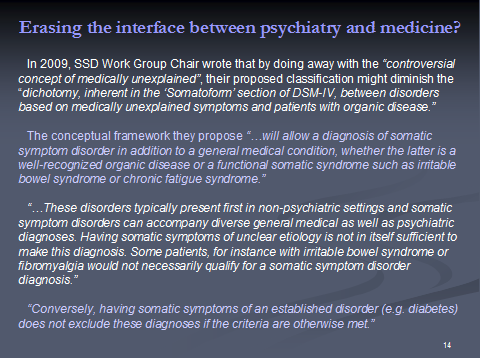
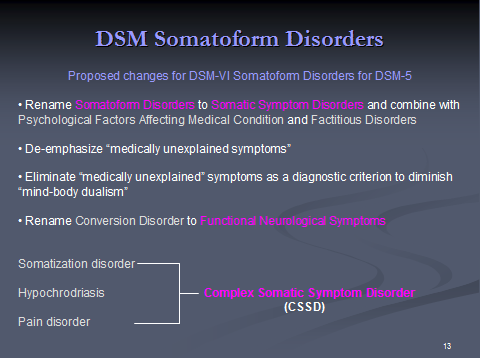
"Please find below a list of disorders that are currently proposed for the diagnostic category, Somatic Symptom Disorders. This category contains diagnoses that were listed in DSM-IV under the chapter of Somatoform Disorders. The Somatic Symptom Disorders Work Group has been responsible for addressing these disorders. Among the work group's recommendations is the proposal to rename this category Somatic Symptom Disorders. Because the current terminology for somatoform disorders is confusing and because somatoform disorders, psychological factors affecting medical condition, and factitious disorders all involve presentation of physical symptoms and/or concern about medical illness, the work group suggests renaming this group of disorders Somatic Symptom Disorders. In addition, because of the implicit mind-body dualism and the unreliability of assessments of "medically unexplained symptoms," these symptoms are no longer emphasized as core features of many of these disorders. Since Somatization Disorder, Hypochondriasis, Undifferentiated Somatoform Disorder, and Pain Disorder share certain common features, namely somatic symptoms and cognitive distortions, the work group is proposing that these disorders be grouped under a common rubric called Complex Somatic Symptom Disorder. Furthermore, the diagnosis of Factitious Disorder can now be found under the diagnostic chapter Other Disorders. We appreciate your review and comment on these disorders.
J 00 Complex Somatic Symptom Disorder Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=368
J 01 Simple Somatic Symptom Disorder Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=491
J 02 Illness Anxiety Disorder Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=10
J 03 Functional Neurological Disorder (Conversion Disorder) Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=8
J 04 Psychological Factors Affecting Medical Condition Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=387
J 05 Other Specified Somatic Symptom Disorder
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=541
J 06 Unspecified Somatic Symptom Disorder
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=12
----------
Revised proposals for criteria for CSSD:
J 00 Complex Somatic Symptom Disorder:
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=368
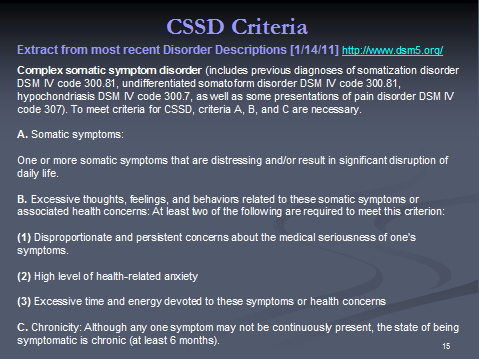
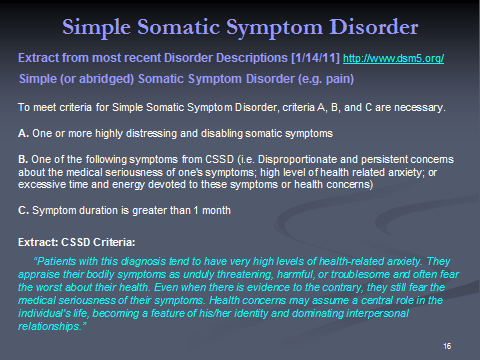
The key "Disorder Description" PDF document has undergone some revisions (highlighted in yellow) since the last version (which was dated January 2011) and is now dated "DRAFT April 18, 2011". There are no highlighted changes for the sections for "Complex Somatic Symptom Disorder" (CSSD) or the more recent, additional proposal for a category called "Simple Somatic Symptom Disorder" (SSSD).
It is this latest version of the PDF that should be referred to and not the version that was published last year at the time of the first public review and feedback.
PDF: "Somatic Symptom Disorders"
http://www.dsm5.org/Documents/Somatic/Somatic Symptom Disorders description April 18, 2011.pdf
Rationale for
J 00 Complex Somatic Symptom Disorder:
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=368#
The key "Justification of Criteria" Rationale PDF document has undergone some revisions (highlighted in yellow) since the last version and is now dated "DRAFT 4/18/11". Again, there are no highlighted changes for the section for "Complex Somatic Symptom Disorder" or "Simple Somatic Symptom Disorder".
Again, it is this latest version of the PDF that should be referred to and not the version that was published last year at the time of the first public review and feedback.
http://www.dsm5.org/Documents/Somatic/DSM Validity Propositions 4-18-11.pdf
The link for the "J01 Simple Somatic Symptom Disorder" page with criteria is here:
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=491
I shall be posting this information on my Dx Revision Watch site, later today, together with the two key PDF documents, and have also posted on selected Facebook sites.
Other than that, because of personal commitments I am not going to be in a position, this year, to undertake awareness raising for this second public DSM-5 draft criteria on international forums.
If you want to see (or remind yourself) what comments were submitted last year, copies of international patient organization submissions for the first DSM-5 public and stakeholder review are collated on this page of my site, together with selected patient and advocate submissions:
DSM-5 Submissions: http://wp.me/PKrrB-AQ or http://wp.me/PKrrB-AQ
Patient organisations, professionals and advocates submitting comments in this second DSM-5 draft proposal review process are once again invited to provide me with copies of their submissions for publication on my site.
Last year, registration was required in order to submit comment via the DSM-5 Development website and you can register to submit comment to the "Somatic Symptom Disorders" Work Group on this page:
http://www.dsm5.org/proposedrevision/Pages/SomaticSymptomDisorders.aspx
A third review and feedback period is currently scheduled for January-February 2012, for two months, following field trials and revisions.
Suzy Chapman
May be reposted in full or in part if source credited
I am resurrecting the existing DSM-5 thread in order that extensive previous material and comment is not lost. There was also discussion of DSM-5 on a second thread, here:
http://forums.phoenixrising.me/showthread.php?3062-DSM5-Ticket-back-to-Reevesville/page17
Please note that for a number of reasons, I no longer participate in these forums and I will not be monitoring this thread and won't be available to discuss the DSM-5 issue but I did feel that readers should be alerted to the following:
ALERT: The second Public Review of draft proposals for criteria and structure for DSM-5 is now open and runs from May to 15th June
This information was posted on Co-Cure mailing list, yesterday:
http://listserv.nodak.edu/cgi-bin/wa.exe?A2=ind1105a&L=co-cure&T=0&F&S&P=2584
Two attachments provided at foot of post.
Yesterday, 4 May, the American Psychiatric Association (APA) announced that a second public review period will run from May to 15 June. This is a revision of its Timeline, as it had stood in March, which had scheduled a public review exercise for August to 30 September.
There has been some media coverage of the APA's announcement here:
http://www.medpagetoday.com/Psychiatry/DSM-5/26275
http://thechart.blogs.cnn.com/2011/05/04/psychiatry-bible-structure-overhauled/
The DSM-5 site was updated yesterday with announcements and revised proposals (dated May 4, 2011) across all categories.
The current review period closes on 15th June - just six weeks away.
Note that this is a public and stakeholder review and feedback exercise and not restricted to professionals or members of the American Psychiatric Association.
There is a Task Force announcement here:
http://www.dsm5.org/Pages/Default.aspx
"What Specifically Has Changed on This Site?
"You will notice several changes to this Web site since we first launched in February 2010. Numerous disorders contain updated criteria...
"...Is There Opportunity to Provide Further Comments?
"At this time, we are asking visitors to review and comment on the proposed DSM-5 organizational structure and criteria changes. Please note that the current commenting period will end on June 15, 2011. It is important to remember that the proposed structure featured here is only a draft. These proposed headings were reviewed by the DSM-5 Task Force in November 2010...
"...The content on this site will stay in its current form until after completion of the DSM-5 Field Trials, scheduled to conclude later this year. Following analysis of field trial results, we will revise the proposed criteria as needed and, after appropriate review and approval, we will post these changes on this Web site. At that time, we will again open the site to a third round of comments from visitors, which will be systematically reviewed by each of the work groups for consideration of additional changes. Thus, the current commenting period is not the final opportunity for you to submit feedback, and subsequent revisions to DSM-5 proposals will be jointly informed by field trial findings as well as public commentary.
"We look forward to receiving your feedback during the coming weeks and appreciate your participation in this important process."
There are brief notes on the proposed DSM-5 Organizational Structure here:
http://www.dsm5.org/proposedrevision/Pages/proposed-dsm5-organizational-structure.aspx
The Recent updates page is here:
http://www.dsm5.org/Pages/RecentUpdates.aspx
The latest revisions for "Somatic Symptom Disorders" are here:
http://www.dsm5.org/ProposedRevision/Pages/SomaticSymptomDisorders.aspx
"Somatic Symptom Disorders
"Please find below a list of disorders that are currently proposed for the diagnostic category, Somatic Symptom Disorders. This category contains diagnoses that were listed in DSM-IV under the chapter of Somatoform Disorders. The Somatic Symptom Disorders Work Group has been responsible for addressing these disorders. Among the work group's recommendations is the proposal to rename this category Somatic Symptom Disorders. Because the current terminology for somatoform disorders is confusing and because somatoform disorders, psychological factors affecting medical condition, and factitious disorders all involve presentation of physical symptoms and/or concern about medical illness, the work group suggests renaming this group of disorders Somatic Symptom Disorders. In addition, because of the implicit mind-body dualism and the unreliability of assessments of "medically unexplained symptoms," these symptoms are no longer emphasized as core features of many of these disorders. Since Somatization Disorder, Hypochondriasis, Undifferentiated Somatoform Disorder, and Pain Disorder share certain common features, namely somatic symptoms and cognitive distortions, the work group is proposing that these disorders be grouped under a common rubric called Complex Somatic Symptom Disorder. Furthermore, the diagnosis of Factitious Disorder can now be found under the diagnostic chapter Other Disorders. We appreciate your review and comment on these disorders.
J 00 Complex Somatic Symptom Disorder Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=368
J 01 Simple Somatic Symptom Disorder Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=491
J 02 Illness Anxiety Disorder Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=10
J 03 Functional Neurological Disorder (Conversion Disorder) Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=8
J 04 Psychological Factors Affecting Medical Condition Updated May 4, 2011
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=387
J 05 Other Specified Somatic Symptom Disorder
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=541
J 06 Unspecified Somatic Symptom Disorder
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=12
----------
Revised proposals for criteria for CSSD:
J 00 Complex Somatic Symptom Disorder:
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=368
The key "Disorder Description" PDF document has undergone some revisions (highlighted in yellow) since the last version (which was dated January 2011) and is now dated "DRAFT April 18, 2011". There are no highlighted changes for the sections for "Complex Somatic Symptom Disorder" (CSSD) or the more recent, additional proposal for a category called "Simple Somatic Symptom Disorder" (SSSD).
It is this latest version of the PDF that should be referred to and not the version that was published last year at the time of the first public review and feedback.
PDF: "Somatic Symptom Disorders"
http://www.dsm5.org/Documents/Somatic/Somatic Symptom Disorders description April 18, 2011.pdf
Rationale for
J 00 Complex Somatic Symptom Disorder:
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=368#
The key "Justification of Criteria" Rationale PDF document has undergone some revisions (highlighted in yellow) since the last version and is now dated "DRAFT 4/18/11". Again, there are no highlighted changes for the section for "Complex Somatic Symptom Disorder" or "Simple Somatic Symptom Disorder".
Again, it is this latest version of the PDF that should be referred to and not the version that was published last year at the time of the first public review and feedback.
http://www.dsm5.org/Documents/Somatic/DSM Validity Propositions 4-18-11.pdf
The link for the "J01 Simple Somatic Symptom Disorder" page with criteria is here:
http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=491
I shall be posting this information on my Dx Revision Watch site, later today, together with the two key PDF documents, and have also posted on selected Facebook sites.
Other than that, because of personal commitments I am not going to be in a position, this year, to undertake awareness raising for this second public DSM-5 draft criteria on international forums.
If you want to see (or remind yourself) what comments were submitted last year, copies of international patient organization submissions for the first DSM-5 public and stakeholder review are collated on this page of my site, together with selected patient and advocate submissions:
DSM-5 Submissions: http://wp.me/PKrrB-AQ or http://wp.me/PKrrB-AQ
Patient organisations, professionals and advocates submitting comments in this second DSM-5 draft proposal review process are once again invited to provide me with copies of their submissions for publication on my site.
Last year, registration was required in order to submit comment via the DSM-5 Development website and you can register to submit comment to the "Somatic Symptom Disorders" Work Group on this page:
http://www.dsm5.org/proposedrevision/Pages/SomaticSymptomDisorders.aspx
A third review and feedback period is currently scheduled for January-February 2012, for two months, following field trials and revisions.
Suzy Chapman