Here an interesting update about my Ambroxol trial.
It happens that even without T3, Ambroxol makes my brain very sleepy and my muscle weaked.
I took Idebenone (a drug that have already helped me in the past in association with it, and bingo! it rescued my brain within an hour, but not my muscles)
I did it two days to see if this effect can be reproduced and it does.
I investigated about what could explain these effects.
I can't find anything about Ambroxol induced sleepiness and weakness, so I may be special (I already know this!), but I found that
Idebenone may be an ANO1 inhibitor, and that
ANO1 activation in the brain induces artery vasocontriction. This means that ANO1 inhibition in the brain will probably induce vasodilatation, same as Nimodipine, a calcium channel blocker that have shown to help some ME/CFS patients here on PR!
Inhibition of ANO1/TMEM16A Chloride Channel by Idebenone and Its Cytotoxicity to Cancer Cell Lines
Abstract
The expression levels of anoctamin 1 (ANO1, TMEM16A), a calcium-activated chloride channel (CaCC), are significantly increased in several tumors, and inhibition of ANO1 is known to reduce cell proliferation and migration. Here, we performed cell-based screening of a collection of natural products and drug-like compounds to identify inhibitors of ANO1. As a result of the screening, idebenone, miconazole and plumbagin were identified as novel ANO1 inhibitors. Electrophysiological studies showed that idebenone, a synthetic analog of coenzyme Q10, completely blocked ANO1 activity in FRT cells expressing ANO1 without any effect on intracellular calcium signaling and CFTR, a cAMP-regulated chloride channel. The CaCC activities in PC-3 and CFPAC-1 cells expressing abundant endogenous ANO1 were strongly blocked by idebenone. Idebenone inhibited cell proliferation and induced apoptosis in PC-3 and CFPAC-1 cells, but not in A549 cells, which do not express ANO1.
These data suggest that idebenone, a novel ANO1 inhibitor, has potential for use in cancer therapy.
ANO1 inhibitors are potentially used to relax uterus:
Functional comparison of anoctamin 1 antagonists on human uterine smooth muscle contractility and excitability
Abstract
Background: Pre-term birth is a major health care challenge throughout the world, and preterm labor represents a potentially reversible component of this problem. Current tocolytics do not improve preterm labor beyond 48 h. We have previously shown that anoctamin 1 (ANO1) channel blockade results in relaxation of pre-contracted human uterine smooth muscle (USM). Three drug classes with reported medicinal effects in humans also have members with ANO1 antagonism. In this study, we compared the ability of representatives from these 3 classes to reduce human USM contractility and excitability.
Objective: This study sought to examine the comparative potency of 3 ANO1 antagonists on pregnant human USM relaxation, contraction frequency reduction, inhibition of intracellular calcium release and membrane hyperpolarization.
...
Conclusion: While all 3 ANO1 antagonists attenuate pregnant human uterine tissue contractility and excitability, BB is the most potent tocolytic drug. Our findings may serve as a foundation for future structure-function analyses for novel tocolytic drug development.
Introduction...
One potential tocolytic target is the calcium-activated chloride channel (CaCC) family member anoctamin 1 (ANO1). CaCC currents have long been recognized as important modulators of smooth muscle excitability (
7,
8,
9). These channels are voltage-gated and responsive to elevations in intracellular calcium levels, making them uniquely suited to participate in excito-mechanical coupling and action potential (AP) generation in smooth muscle tissues (
7,
10)
...
Molecular identification of the ANO1 channel as a CaCC was not established until recently (
17,
18,
19). The ANO1 channel is now known to play important roles in various cell types including airway and intestinal epithelial cells, smooth muscle cells, intestinal pacemaker cells, and sensory neurons (
20,
21,
22,
23)
Local coupling of TRPC6 to ANO1/TMEM16A channels in smooth muscle cells amplifies vasoconstriction in cerebral arteries
Abstract
Anoctamin-1 [ANO1, also known as transmembrane protein 16A (TMEM16A)] is a Ca2+-activated Cl− channel expressed in arterial myocytes that regulates membrane potential and contractility. Signaling mechanisms that control ANO1 activity in arterial myocytes are poorly understood.
In cerebral artery myocytes, ANO1 channels are activated by local Ca2+ signals generated by plasma membrane nonselective cation channels, but the molecular identity of these proteins is unclear. Arterial myocytes express several different nonselective cation channels, including multiple members of the transient receptor potential receptor (TRP) family. The goal of this study was to identify localized ion channels that control ANO1 currents in cerebral artery myocytes.
....
These data indicate that TRPC6 channels generate a local intracellular Ca2+ signal that activates nearby ANO1 channels in myocytes to stimulate vasoconstriction.
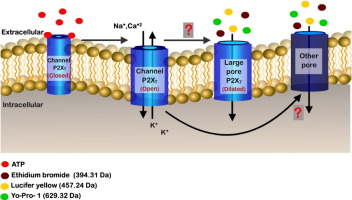
I have to look into puringergic receptors...
I guess there must be a chapter about it in your book, more and more scientific studies are released about the P2X receptors/channels, it's amazing to have all these new informations available about ion channels!