SilverbladeTE
Senior Member
- Messages
- 3,043
- Location
- Somewhere near Glasgow, Scotland
Which would beg the question, what exactly were CBT and GET treating?
Underdevelopment of the frontal lobe of the psychs' wage packet?


Which would beg the question, what exactly were CBT and GET treating?
========I asked the Lancet editors what the closing date is, and their response was:
----------
----------The two-week deadline for submission of Correspondence refers to the date
the relevant article was first published, so in this case the date of online
publication. You should therefore submit your letter as soon as possible.
We will still consider submissions received after this deadline, but we may
not be able to give them priority when compared to letters received within
the allotted timeframe.
It was published on 18 Feb, so by my calculations this makes the deadline
the 4th Mar, which is tomorrow!
The last days I have "fanned out" (got tired). Today I am just trying to get the day pass by without suffering to much.
Thank you for all your comments. I have learned a lot about the PACE trial.
I think one can critic the trial because the patient selection was a sort of "special" because as I understood the patients that wanted to participate in the trial was positive to it. I guess very few "true" ME patients signed up for the trial. Therefore one can question if this would be applicable to Canadian criteria ME/CFS patients. Patients with moderate to severe ME with post exertional malaise may not be present at all in the cohort.
The patients only had to be "tired" as required by the Oxford critieria.
The sub-cohort of the study with patients said to fulfil the London criteria seems to have been selected by patient filled in forms only. I think it is important that a specialist sets the diagnosis. For a patient it may e.g. be difficult to understand what is "post exertional malaise". Also one can question the neutrality of the researchers as they have a firm reputation of beeing "militant supporters of the psychiatric school". Of course they did not included objective measurements including biomedical parameters. Some say some of these researchers have connections to insurance companies that do not have to pay for psychiatric conditions. Peter White, Trudie Chalder and Michael Sharpe are well known for their persistent policy of trying to pretend that ME is a psychiatric, psychosomatic or psychosocial condition. They stretch the results of their studies impossibly far. Data that is inconclusive or showing subjective marginal effects of CBT or GET are stretched in the conclusions to be highly effective. They mislead, one has to call it lying, when they use the term CFS for fatigued patients in general. Actually, in science precision and clarity is important, but for "Peter White gang" obfuscation is part of their agenda. One would believe they rather belong to the world of wizardry than to the world of science.
Where comes the will from to confuse researchers and people in general by using a term that already has a definition?
The exercise program was ultra light. Maybe the authors made the program ultra light on purpose in order to make sure the results were positive and few patients reporting severe adverse reactions. Again, remember that the patients in the study were quite fit in comparison to a regular ME patient.
Ten percent of the patients got worse during the study. Thirty percent in the intervention group(s) got better. But fifteen percent of the non intervention group also got better. That is only a further 15% got better from the interventions.
The "getting better" was very slight, and the statements in the Lancet paper are misleading and false. The data does not support "getting a normal function". Such statements are lies from my point of view.
If one assumes that depressed patients were in the cohort, one an understand they got better. Depression has a natural history of about a year. That is the time of the study. A depressed patient that is supported and does something he believes in, will probably get an immediate effect on well being.
Finally I think it might be possible that some patients with a ME diagnosis may get better from stepwise increased activity. I believe it depends on the sub-group, the level of invalidity and in what phase on is in the disease. According to statistics I have seen and stories about ME patients it seems that there are some that indeed get better from stepwise increased activity. The point still is that ME is a somatic condition and the researchers that have performed the study does everything they can to pretend it is not. This may lead to less money for ME biomedical research. Many (the majority) patients in Sweden complain about physicians that say ME does not exist and suggest them to exercise. Some patients have had permanent exacerbations as a result of pushing them selves with the wish it will make them healthy. Statistics collected by patients organizations confirms that GET is a treatment that make a few feel better, but that a majority feel worse. Actually, most patients push in their daily life already. Personal hygiene, cleaning the house, cooking food and buying food is already exercise them. The short times of feeling better is precious to patients. During this time they want to do things that they have been longing to do for maybe days. One can understand that these patients are not very interesting to use this time to "non productive" exercise. For a patient that rarely get out of the house, each week is precious. There are only 50 weeks during a year. If the patient can get out to do errands once a week, then one can understand that one has to ration the activities to the most important ones. The patients are often frustrated to the lack of energy and the inability to move the life forwards. One can understand that they do not want to participate in GET. Also, patients have created cooping skills on their own over time. A great deal of the patients have gotten worse during the time the medical physicians did not suspect ME. They may already have participated in CBT without improving. Merely, the patient has come to the understanding that either the physician or the therapist does not have a clue what the patient has.
In a big study with over 300 patients, 48% reported getting worse from GET. A study made among patients with severe ME, 82% reported getting worse from GET. Some of them actually got severe ME as a result of GET.
http://www.investinme.org/IIME Campaigning-CBT-GET-002.htm
According to a patient organisation in UK 56% got worse of GET.
http://www.meassociation.org.uk/wp-content/uploads/2010/09/2010-survey-report-lo-res10.pdf
Open online studies have their limits and risks because anyone can reply to them, but according to a survey GET makes most patients worse.
http://curetogether.com/blog/2011/0...helps-patients-with-chronic-fatigue-syndrome/
http://curetogether.com/Chronic-Fatigue-Syndrome/treatments/
You may repost or use my draft of comments, preferably without my name.
Conflicts of interest
PDW has done voluntary and paid consultancy work for the UK
Departments of Health and Work and Pensions and Swiss Re
(a reinsurance company). DLC has received royalties from Wiley. JB was
on the guideline development group of the National Institute for Health
and Clinical Excellence guidelines for chronic fatigue syndrome and
myalgic encephalomyelitis and has undertaken paid work for the
insurance industry. GM has received royalties from Karnac. TC has done
consultancy work for insurance companies and has received royalties
from Sheldon Press and Constable and Robinson. MB has received
royalties from Constable and Robinson. MS has done voluntary and paid
consultancy work for government and for legal and insurance
companies, and has received royalties from Oxford University Press.
ALJ, BA, HLB, LVC, JCD, KAG, LP, MM, PM, HO, RW, and DW declare
that they have no confl icts of interests.
If you're improving, you may naturally exercise more. That's not the same as exercise getting you better, etc.Free full text: http://pediatrics.aappublications.org/cgi/content/full/124/1/189
Chronic fatigue syndrome after infectious mononucleosis in adolescents.
Pediatrics. 2009 Jul;124(1):189-93.
Katz BZ, Shiraishi Y, Mears CJ, Binns HJ, Taylor R.
Department of Pediatrics, Division of Infectious Diseases, Northwestern University Feinberg School of Medicine and Children's Memorial Hospital, Chicago, Illinois 60614, USA. bkatz@northwestern.edu
Abstract
OBJECTIVE: The goal was to characterize prospectively the course and outcome of chronic fatigue syndrome in adolescents during a 2-year period after infectious mononucleosis.
METHODS: A total of 301 adolescents (12-18 years of age) with infectious mononucleosis were identified and screened for nonrecovery 6 months after infectious mononucleosis by using a telephone screening interview. Nonrecovered adolescents underwent a medical evaluation, with follow-up screening 12 and 24 months after infectious mononucleosis. After blind review, final diagnoses of chronic fatigue syndrome at 6, 12, and 24 months were made by using established pediatric criteria.
RESULTS: Six, 12, and 24 months after infectious mononucleosis, 13%, 7%, and 4% of adolescents, respectively, met the criteria for chronic fatigue syndrome. Most individuals recovered with time; only 2 adolescents with chronic fatigue syndrome at 24 months seemed to have recovered or had an explanation for chronic fatigue at 12 months but then were reclassified as having chronic fatigue syndrome at 24 months. All 13 adolescents with chronic fatigue syndrome 24 months after infectious mononucleosis were female and, on average, they reported greater fatigue severity at 12 months. Reported use of steroid therapy during the acute phase of infectious mononucleosis did not increase the risk of developing chronic fatigue syndrome.
CONCLUSIONS: Infectious mononucleosis may be a risk factor for chronic fatigue syndrome in adolescents. Female gender and greater fatigue severity, but not reported steroid use during the acute illness, were associated with the development of chronic fatigue syndrome in adolescents. Additional research is needed to determine other predictors of persistent fatigue after infectious mononucleosis.
Lots of people improve with time as this study shows:
If you're improving, you may naturally exercise more. That's not the same as exercise getting you better, etc.
I feel like we've barely scratched the surface.
Personally, I was hoping Pace would bring some genuinely useful data for helping me understand how I should behave. However, the way they've spun the figures for 'back to normal' really makes it impossible to believe any of the results they've presented.
We propose that a clinically important
difference would be between 2 and 3 times the improvement
rate of SSMC.
I wonder if they've reflected upon why their own minds misled them about the efficacy of the treatments they're promoting. I wonder if they're concerned about their own cognitive distortions having caused any other problems for their patients?
But seriously, I think they did believe they had ME all sewn up with CBT & GET and what I find so maddening is that rather than reflecting on the true meaning of the results they are now talking about better CBT. Really, this study should be the biopsychosocial model's nemesis, but I suspect that the plan is for business as usual.
I think they are still in some shock and desperately trying to figure out how to salvage something more than a minority of unusually selected patients report some improvement on some limited and not entirely appropriate subjective measures, using highly manipulated unreal definitions of 'recovery', and with no supporting evidence from objective measures.
I know it is cold comfort to patients right now, but I still cannot see them and their model surviving this scientifically.
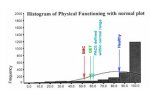
View attachment 5115
sorry it's so small (click to enlarge slightly).
nb for the working age population that would be the relevant comparison for PACE, the 'tail' would be even smaller (and of course the tail is made up of the sick).
This is taken from page 9 of the open access article (notations added by me): Bowling SF-36 normative data
Although the article and picture are freely available there may be copyright issues so please don't reproduce this pic.
Nicely put. However, i'm not sure I quite share your optimism that their model will simply fold beneath the weight of evidence, though it surely it would it an ideal world. I think working out how to expose the real meaning of PACE, both in the media and in the scientific world, is a huge challenge for us all. Letters to the Lancet were a first step and I'm not quite sure where we go from here. Though, for me, the next step is more sifting through the PACE trial to really understand what's going on.
That is an interesting histogram, it puts the trial results into perspective if they are shown compared to the normal population.
I want to volunteer to help them with their own "false illness beliefs"....I wonder if they've reflected upon why their own minds misled them about the efficacy of the treatments they're promoting. I wonder if they're concerned about their own cognitive distortions having caused any other problems for their patients?