https://www.whatdotheyknow.com/request/distinguishing_between_cfsme_who
18 November 2012
FOI, Mr Courtney
Extract:
[...]
As to the classification of CFS/ME within the guideline, we acknowledge
that many different potential causes have been investigated – including
neurological, endocrine, immunological, genetic, psychiatric and
infectious – but the diverse nature of the symptoms cannot yet be fully
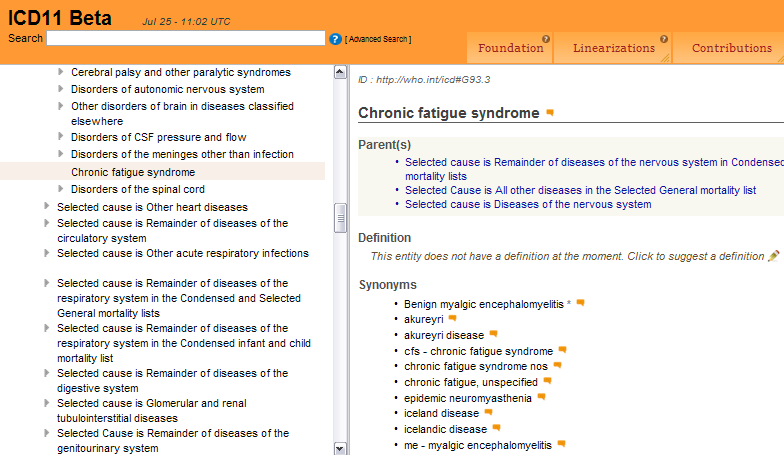
explained. As you are aware the guideline recognises that the World Health
Organization (WHO) classifies CFS/ME as a neurological illness. Some
members of the Guideline Development Group felt that, until further
research identifies its cause and how it develops, the guideline should
recognise this classification. So while it is generally recognised that
CFS/ME is heterogeneous, the evidence did not allow distinctions between
sub-groups with regard to diagnosis or management of the condition. This
assessment can be found in Section 1 of the full guideline document which
can be downloaded from the NICE website.
The issue of the classification of the disease was commented on by
stakeholders during the public consultation as this had not been included
in the first draft. In response to feedback received we revised the text
in the guideline to include reference to the World Health Organisation
(WHO) classification ICD10 as G93.3. In the [5] general stakeholder
comments you can read the feedback from stakeholders on this issue, this
feedback includes information on correspondence that external stakeholders
have had with the WHO regarding the classification of the disease in
ICD10.