@Garz which tests turned up
Positive to confirm your tick bourne illness?
as you know there are no ideal tests for lyme - and due to this fact the picture gets pretty complex quite quickly.
so, rather than being put off by the complexity, i did a lot of research into available testing;
for lyme -
about the best test lab in Europe is Armin Labs in Germany
they do not make any of their own tests - but use accredited tests from accredited manufacturers
they have a test called Tickplex made by a Finnish company called Tezted.
its notable because it uses antigens from European strains of borrelia as well as borrelia burgdorferi sensu stricto
it also has antigens for round bodies or persister forms of the bacteria - which are different
(as opposed to most lyme serologic tests - that use only lab strains of USA sourced borrelia species eg Borrelia Burgdorferi B31 strain - which was not taken from a human patient, and only motile forms - which is not how they live in the body)
i read the validation studies the Finish manufacturer published in Nature and i contacted the lead author to discuss them to ensure i fully understood the sensitivity ad specificity calculations.
Based on this i found a positive tests, such as mine, with both IgG and IgM positive had above 90% positive diagnostic value.
this combined with my extremely lyme-like symptom pattern and an extremely low CD57+ count (often present in chronic Lyme ) raised the likelihood of a true positive higher. presence of another arthropod borne infection - see below - raises the likelihood further still.
it should be noted that many lyme tests are still negative in infected persons - there are many reasons for this that would take too long to go into here - but for instance there are in the wild many more species of borrelia than we have tests for and more are being found all the time, something like 20 species so far - and also a further 15 or so Relapsing Fever type borrelia species - which may present exactly like lyme disease. this may be the reason for many people having partial positive results on western blots.
Its also not well appreciated by the patient population that according to published studies - the instances of false negatives are 5-8x higher than false positives. So there is dramatic asymmetry in testing – such that a person with a positive test result and a negative test result would do well to consider the false negative at least 5x more likely( rather than an instinctive - “well, I had one positive result ad one negative result - so its 50/50”)
bartonella testing is even more problematic
- serologic testing is so poor it has been withdrawn from clinical use by the UK NHS. the reasons for this are not fully researched - but its clear that serology is positive in only a small % of those demonstrated to be infected by other means. immune suppression by the infection - and wide diversity in bartonella species and within species genotypes and their resulting antigens both have significant evidence supporting them as possible explanations. If your body has made antibodies to the specific phenotype antigen that the test uses - you may still test positive - but studies indicate this is only in a small number of cases - perhaps 25% max
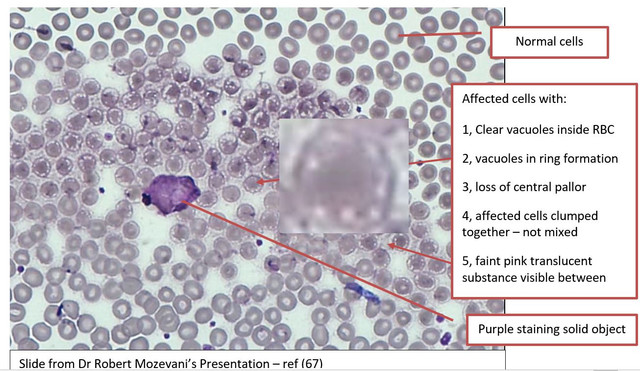
- standard PCR testing is also very low sensitivity - mainly because the organism is not evenly distributed in the blood of infected persons as is typically assumed (see image below from bartonella specialist and Harvard educated MD - Robert Mozeyani) -so is not reliably found in the sample is a known issue.
the short answer is - after years of digging - i finally diagnosed myself with bartonella based on microscopy.
to explain further - the standard mantra in infectious disease circles is that bartonella is too small to visualise directly with light microscopy, which is kind of true, and as a result you will not find the following information in any medical test book.
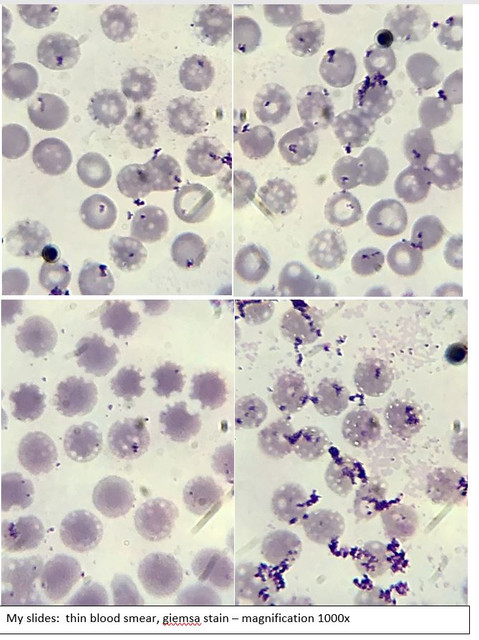
however Bartonella is known to reside inside red blood cells - and when doing so it creates a vacuole around itself ( this part is well documented in the scientific literature) - what is not commonly understood is that when the red blood cells are stained with an appropriate dye - the vacuoles can be clearly visualised using a laboratory grade microscope, as a ring of clear spots around the periphery of infected red blood cells. no other organism infects red blood cells and causes this pattern and as a result this presentation is 100% diagnostic.
it is time consuming and not all slides will show infection - due to the clumping of infected cells described by Dr Mozeyani - so several slides must be carefully inspected.
the advantages are
- this is a direct test method - infection can be physically visualised - not a secondary marker
- it requires no patient immune response / antibodies to be formed ( immune responses are variable)
- or selection of test antigens to match patient species or strain - all bartonella present this way.
other signs and symptoms in the slides can also support the diagnosis -
- prolific coloured biofilms are visualised with the same technique ( bartonella causes fibrin deposits )
- distortions of red blood cell structures / membranes, also indicates intracellular infection
- platelet aggregation can also be seen - again indicative of infection / inflammation
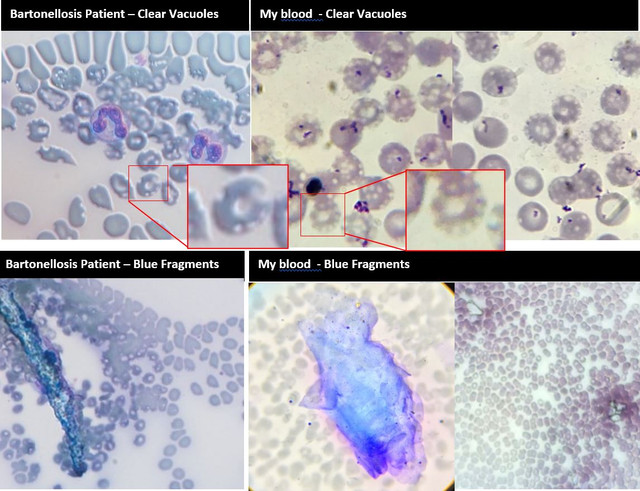
the below slide is an image of the blood of a bartonella infected patient of Dr Mozeyani
note the cluster of red blood cells with rings of clear dots (vacuoles) inside them
i tested negative for bartonella via conventional serology – even at specialist Tick born testing labs ( se issues with testing above ) and yet my blood had prolific infection with bartonella.
 [/url
[/url
]
I also had the other signs visible in bartonella patients – blue staining fragments of fibrin/biofilm and platelet aggregation
 [/url
[/url
]
This form of microscopy could be of great benefit to bartonella sufferers around the world - as other forms of testing are either so poor as to be almost a total waste of time - or so expensive they are out of reach of many who need it. As a result, i am contemplating setting up a testing service to provide it direct to patients via mail order.
@Garz I get the vibration also- did not know thar was a symptom of bartinella. Do you know what the mechanism of that might be.
The well-known Yale trained lyme doctor Steven Phillips MD - has presented that he finds this buzzing / vibrating internal sensation - almost unique to his bartonella patients.
anecdotally - you will see it mentioned by many diagnosed bartonella sufferers in Lyme / Bart support groups support groups
eg https://www.healingwell.com/community/default.aspx?f=30
and
https://www.facebook.com/groups/1104493829902071/
research is lacking on the mechanism that causes it - but it should be noted that bartonella is known to cluster around nerve fibres in tissues in infected persons (see confocal laser microscopy work by Marna Ericson PhD on tissue biopsies) - and is known to cause inflammation wherever it resides.
bartonella is also known to cause neuropathies in many of the persons it infects - everything from palsy of nerves in face or arms to gastroparesis, to small fibre neuropathies. neuropathies can present as pain, burning, tingling, numbness or buzzing sensations - so i would guess that something like this is likely at work.
this may be a direct effect or an auto-immune mediated effect - as bartonella is known for causing auto-immune disorders in infected patients.


 )! When I find the EKG's & my notes, I can explain it better
)! When I find the EKG's & my notes, I can explain it better