Sasha submitted a new blog post:
Get a Ringside Seat for Invest in ME’s 10th International Conference on 29 May
Sasha and Simon preview the attractions and tells you how you can watch it unfold ...
This Friday, 29 May sees the tenth International ME Conference put on by UK research charity Invest in ME (IiME) in London. The day-long conference will include 220 participants from 17 countries and will be attended by researchers, clinicians and patients.

The conference has grown from small beginnings to being one of the most important events on the international ME research calendar, not least because it’s preceded by a two-day, invitation-only research colloquium — now in its fifth year — where some of the world’s top ME researchers can put their minds together and make things happen.
IiME used their 2013 colloquium to gather researchers who might be interested in a UK replication of the exciting rituximab trial results seen in Norway and their initiative paid off.
A University College London team, led by Jo Cambridge and advised by Emeritus Professor Jonathan Edwards, took up the challenge to do a UK trial and IiME began a wildly successful, ongoing crowdfund for the research which has raised a spectacular £380,000 ($590,000, €530,000) so far.
So, we can expect big things. The colloquium happens behind closed doors but the conference doesn’t, and Mark Berry from Phoenix Rising will be in the audience, preparing an in-depth article about the research (his 2013 coverage is here, and 2014 here and here). He and others will be tweeting for Phoenix Rising so that you can follow the presentations live.
Professor Olav Mella (left) and Dr. Oystein Fluge
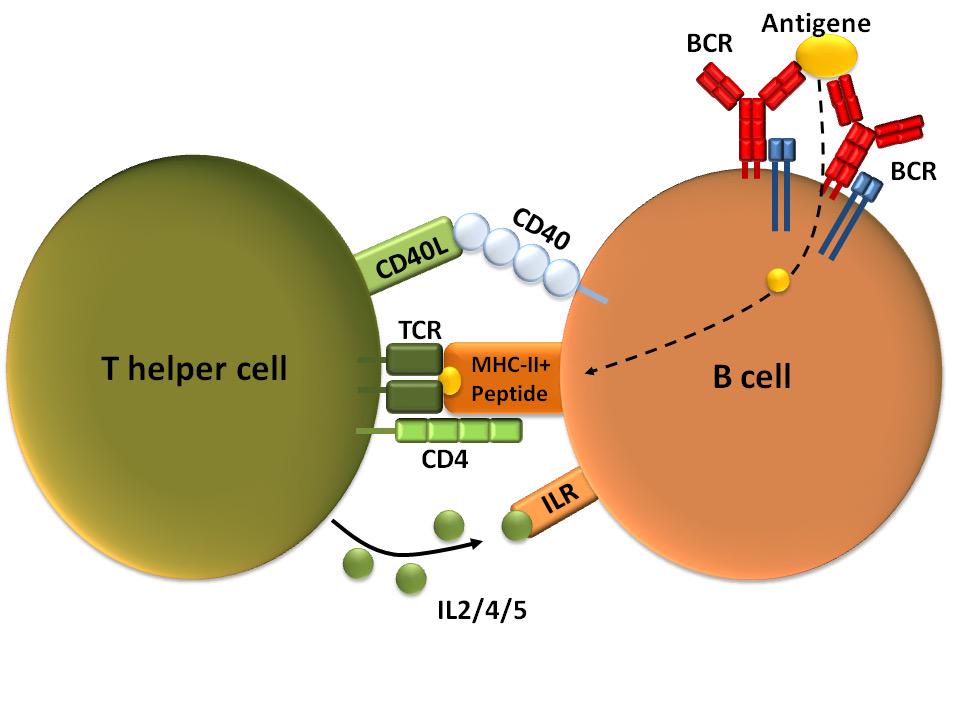
The stars of the show are likely to be Oystein Fluge and Olav Mella with the latest from Norway on the new, multi-centre rituximab trial, with Jo Cambridge reporting on B-cell profiling aimed at identifying likely responders in the forthcoming IiME UK rituximab trial.
Other highlights include John Chia on how enteroviruses might cause ME/CFS, Mady Hornig on markers of immunity and metabolism, Betsy Keller on molecular markers before and after exercise and Louis Nacul on ME/CFS population rates.
There’s also brain-immune communication, proteomics explained, an update from Down Under by Sonya Marshall-Gradisnik, and Amolak Bansal on better diagnosis. Professor Ian Charles will deliver the keynote address, on what a research park can do to solve a chronic illness.
The full programme is as follows:
Until 31 May you can get an ‘early bird’ price on Invest in ME’s DVD of the conference, which will be released in July.
And, of course, feel free to donate to IiME’s research! They have a general biomedical research fund, a rituximab trial fund, and a fund for a study on the gut, looking at the microbiome and gut-wall permeability (‘leaky gut’).
This is a small charity that punches well above its weight and is well worth supporting.
So, we’ve got something to look forward to on Friday — and don't forget to tune in for Phoenix Rising's live tweeting from the ringside.
Let’s hope for a conference to remember!
Phoenix Rising is a registered 501 c.(3) non profit. We support ME/CFS and NEID patients through rigorous reporting, reliable information, effective advocacy and the provision of online services which empower patients and help them to cope with their isolation.
There are many ways you can help Phoenix Rising to continue its work. If you feel able to offer your time and talent, we could really use some more authors, proof-readers, fundraisers, technicians etc. We’d also love to expand our Board of Directors. So, if you think you can help in any way then please contact Mark through the Forums.
And don’t forget: you can always support our efforts at no cost to yourself as you shop online! To find out more, visit Phoenix Rising’s Donate page by clicking the button below.
 Continue reading the Original Blog Post
Continue reading the Original Blog Post
Get a Ringside Seat for Invest in ME’s 10th International Conference on 29 May
Sasha and Simon preview the attractions and tells you how you can watch it unfold ...
This Friday, 29 May sees the tenth International ME Conference put on by UK research charity Invest in ME (IiME) in London. The day-long conference will include 220 participants from 17 countries and will be attended by researchers, clinicians and patients.

IiME used their 2013 colloquium to gather researchers who might be interested in a UK replication of the exciting rituximab trial results seen in Norway and their initiative paid off.
A University College London team, led by Jo Cambridge and advised by Emeritus Professor Jonathan Edwards, took up the challenge to do a UK trial and IiME began a wildly successful, ongoing crowdfund for the research which has raised a spectacular £380,000 ($590,000, €530,000) so far.
So, we can expect big things. The colloquium happens behind closed doors but the conference doesn’t, and Mark Berry from Phoenix Rising will be in the audience, preparing an in-depth article about the research (his 2013 coverage is here, and 2014 here and here). He and others will be tweeting for Phoenix Rising so that you can follow the presentations live.

Professor Olav Mella (left) and Dr. Oystein Fluge
The stars of the show are likely to be Oystein Fluge and Olav Mella with the latest from Norway on the new, multi-centre rituximab trial, with Jo Cambridge reporting on B-cell profiling aimed at identifying likely responders in the forthcoming IiME UK rituximab trial.
Other highlights include John Chia on how enteroviruses might cause ME/CFS, Mady Hornig on markers of immunity and metabolism, Betsy Keller on molecular markers before and after exercise and Louis Nacul on ME/CFS population rates.
There’s also brain-immune communication, proteomics explained, an update from Down Under by Sonya Marshall-Gradisnik, and Amolak Bansal on better diagnosis. Professor Ian Charles will deliver the keynote address, on what a research park can do to solve a chronic illness.
The full programme is as follows:
08.55 Dr. Ian Gibson Conference Opens
09.05 Professor Ian Charles (Keynote Speech) Solving ME: What a Research Park Has to Offer in Resolving a Chronic Disease
09.30 Professor Mady Hornig Markers of Immunity and Metabolism in ME/CFS
10.00 Professor Jonas Bergquist Proteomics in ME/CFS
10.25 Refreshments Break
10.50 Dr. Luis Nacul Incidence and Prevalence of ME
11.15 Dr. Amolak Bansal Diagnosis and Differential Diagnosis: Combining clinic and research
11.45 Professor Sonya Marshall-Gradisnik, Dr Don Staines (To be confirmed) Update from National Centre for Neuroimmunology and Emerging Diseases - NCNED
12.15 IiME Projects Student Researchers: The Next Generation
12.40 Lunch
13.40 Dr. Jo Cambridge B-cell biology and ME/CFS
14.05 Dr. Neil Harrison Immune-Brain Communication and Relationship to Inflammation
14.30 Dr. John Chia ME and Chronic Enterovirus Infection: An Update on pathogenesis.
14.55 Dr. Claire Hutchinson Biomarkers for ME: Visual Processing and ME/CFS
15.20 Refreshments break
15.50 Professor Betsy Keller Molecular markers before/after exercise /Activity guidelines to avoid symptom flares
16.15 Dr. Oystein Fluge, Professor Olav Mella Multi-centre Rituximab Clinical Trial for ME/CFS
17.10 Plenary Will ME Be Treatable/Cured?
17.30 Dr. Ian Gibson Adjourn
09.05 Professor Ian Charles (Keynote Speech) Solving ME: What a Research Park Has to Offer in Resolving a Chronic Disease
09.30 Professor Mady Hornig Markers of Immunity and Metabolism in ME/CFS
10.00 Professor Jonas Bergquist Proteomics in ME/CFS
10.25 Refreshments Break
10.50 Dr. Luis Nacul Incidence and Prevalence of ME
11.15 Dr. Amolak Bansal Diagnosis and Differential Diagnosis: Combining clinic and research
11.45 Professor Sonya Marshall-Gradisnik, Dr Don Staines (To be confirmed) Update from National Centre for Neuroimmunology and Emerging Diseases - NCNED
12.15 IiME Projects Student Researchers: The Next Generation
12.40 Lunch
13.40 Dr. Jo Cambridge B-cell biology and ME/CFS
14.05 Dr. Neil Harrison Immune-Brain Communication and Relationship to Inflammation
14.30 Dr. John Chia ME and Chronic Enterovirus Infection: An Update on pathogenesis.
14.55 Dr. Claire Hutchinson Biomarkers for ME: Visual Processing and ME/CFS
15.20 Refreshments break
15.50 Professor Betsy Keller Molecular markers before/after exercise /Activity guidelines to avoid symptom flares
16.15 Dr. Oystein Fluge, Professor Olav Mella Multi-centre Rituximab Clinical Trial for ME/CFS
17.10 Plenary Will ME Be Treatable/Cured?
17.30 Dr. Ian Gibson Adjourn
Until 31 May you can get an ‘early bird’ price on Invest in ME’s DVD of the conference, which will be released in July.
And, of course, feel free to donate to IiME’s research! They have a general biomedical research fund, a rituximab trial fund, and a fund for a study on the gut, looking at the microbiome and gut-wall permeability (‘leaky gut’).
This is a small charity that punches well above its weight and is well worth supporting.
So, we’ve got something to look forward to on Friday — and don't forget to tune in for Phoenix Rising's live tweeting from the ringside.
Let’s hope for a conference to remember!
Phoenix Rising is a registered 501 c.(3) non profit. We support ME/CFS and NEID patients through rigorous reporting, reliable information, effective advocacy and the provision of online services which empower patients and help them to cope with their isolation.
There are many ways you can help Phoenix Rising to continue its work. If you feel able to offer your time and talent, we could really use some more authors, proof-readers, fundraisers, technicians etc. We’d also love to expand our Board of Directors. So, if you think you can help in any way then please contact Mark through the Forums.
And don’t forget: you can always support our efforts at no cost to yourself as you shop online! To find out more, visit Phoenix Rising’s Donate page by clicking the button below.
Last edited by a moderator: