

uglevod
Senior Member
- Messages
- 220
Antioxidant Supplementation Enhances Bacterial Peritonitis in Mice by Inhibiting Phagocytosis
https://www.researchgate.net/public...eritonitis_in_Mice_by_Inhibiting_Phagocytosis
Antioxidants are known to exhibit numerous health benefits including anti-aging, anti-apoptotic and immuno-stimulatory effects. However, we present the data showing counterproductive effects of therapeutically relevant antioxidants on bacterial clearance by immune system in murine peritonitic model. The antioxidants ascorbic acid (Asc), glutathione (GSH) and N-acetylcysteine (NAC) augmented morbidity and mortality in mice carrying E. coli induced acute bacterial peritonitis. Treatment of peritonitic mice with antioxidants significantly increased their bacterial load in the range of 0.3 to 2 log orders. Antioxidant administration to peritonitic mice resulted in decreased number of macrophages, B cells and dendritic cells at the primary site of infection and increased neutrophil infiltration.
The serum Tumor Necrosis Factor-α levels were also decreased in antioxidant treated peritonitic mice.
In vitro experiments showed that antioxidants reduced phagocytic efficacy of peritoneal macrophages by ≈60-75% and also decreased E. coli induced oxidative burst in macrophages cells.
Taken together our data indicate that the antioxidants increased severity of peritonitis via decreasing the phagocytic efficiency, oxidative burst, TNF- alpha production and increasing neutrophil infiltration.
Based on these results we propose that antioxidant supplementation during the course of bacterial infection is not recommended as it could be detrimental for the host. Besides, the present study underlines the importance of timing and context of antioxidants administration as opposed to indiscriminate usage to gain best possible therapeutic advantage of these redox compounds.
^
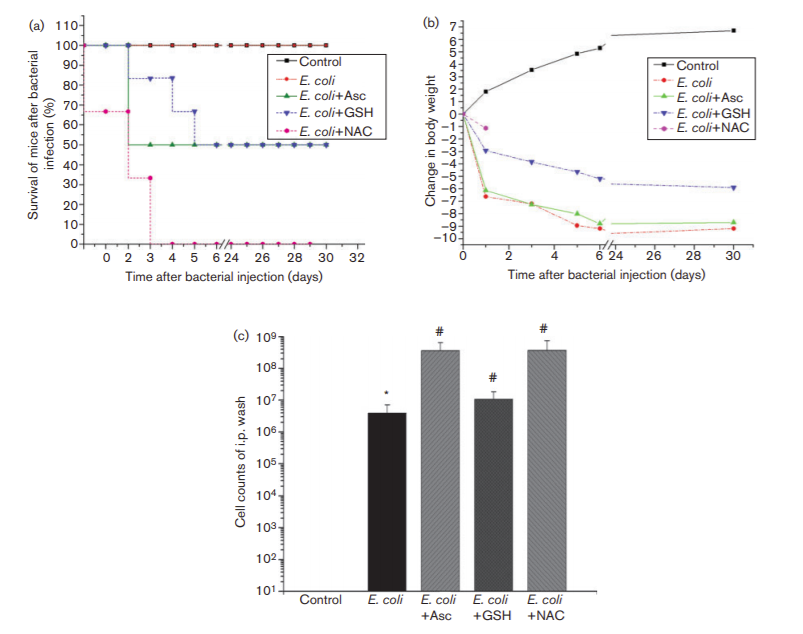
Survival, body weight and peritoneal bacterial load after antioxidant administration in peritonitic mice. (a) Survival of the mice given different treatments over a period of 30 days. The mice were challenged with ~3108 E. coli cells and 500 mg (kg body weight)”1 of one of the antioxidants (GSH/Asc[ascorbic acid]/NAC) through the i.p. route (n56 mice per group). (b) Changes in body weight of the mice during 30 days after injection of E. coli and one of the antioxidants (n56 mice per group). Each data point represents mean±SEM. (c) Changes in peritoneal bacterial load of mice subjected to different combinations of E. coli and antioxidant treatments (n54 mice per group). *P,0.05 compared with the control; #P,0.05 compared with the E. coli-treated group.
Effect of antioxidants on intracellular ROS levels in peritoneal macrophages in vitro
Upon exposure to bacteria, phagocytes produce high levels of ROS by a process called oxidative burst. The bacteria induced alterations in intracellular ROS levels of murine peritoneal macrophages were measured in the presence or absence of exogenously added antioxidants.
...
The decrease in E. coli-induced ROS production was more prominent in macrophages co-incubated with antioxidants compared with those pre-incubated with antioxidants.
...
The present study conceivably proposes that antioxidant administration in animals with bacterial infection could be harmful for the host physiology. This statement is supported by our data that antioxidant administration caused increased bacterial load in the peritonitic mice, ultimately leading to their decreased survival
...
Thus, the antioxidant-mediated decrease in phagocytosis and oxidative burst would disarm the host immune response and thus contribute to the increased bacterial load, leading to higher host mortality. Our proposal is further supported by an independent recent report showing a curcumin-mediated compromised immunological response against invading pathogens in a murine typhoid model (Marathe et al., 2013).
...
Similarly, increased progression of Chlamydia trachomatis infection in the presence of GSH and NAC has been reported previously (Lazarev et al., 2010). Moreover, the presence of supplementary antioxidants at the site of infection could also interfere with the antibody-mediated bacterial killing via the ozonolysis pathway, thereby inhibiting the formation of neutrophil extracellular traps, which facilitate the clearance of bacterial infection from the host’s body (Brinkmann et al., 2004). However, these propositions are yet to be validated experimentally.
...
On the whole, the results of our present study reveal for the first time that antioxidant administration in animals having acute bacterial peritonitis leads to overall deterioration of host conditions. This is the fallout of antioxidant-mediated modulation of three important immunological parameters involved in antibacterial defence:
(i) phagocytic efficacy and oxidative burst;
(ii) neutrophil infiltration and Gr1 expression;
(iii) expression of CD11b, which is a component of complement receptor CR3.
This is an initial but significant step towards understanding the in vivo role of antioxidant supplementation during clearance of bacterial infection. Importantly, we previously established that antioxidants eliminate antibiotic-induced bacterial killing (Goswami et al., 2006, 2007), and our current study indicates that they can also promote bacterial infection by decreasing the capacity of immune cells. Therefore, the knowledge obtained from our previous and present studies strengthens the hypothesis that antioxidants may interfere with the overall clearance of bacterial infections in vivo.
https://www.researchgate.net/public...eritonitis_in_Mice_by_Inhibiting_Phagocytosis
Antioxidants are known to exhibit numerous health benefits including anti-aging, anti-apoptotic and immuno-stimulatory effects. However, we present the data showing counterproductive effects of therapeutically relevant antioxidants on bacterial clearance by immune system in murine peritonitic model. The antioxidants ascorbic acid (Asc), glutathione (GSH) and N-acetylcysteine (NAC) augmented morbidity and mortality in mice carrying E. coli induced acute bacterial peritonitis. Treatment of peritonitic mice with antioxidants significantly increased their bacterial load in the range of 0.3 to 2 log orders. Antioxidant administration to peritonitic mice resulted in decreased number of macrophages, B cells and dendritic cells at the primary site of infection and increased neutrophil infiltration.
The serum Tumor Necrosis Factor-α levels were also decreased in antioxidant treated peritonitic mice.
In vitro experiments showed that antioxidants reduced phagocytic efficacy of peritoneal macrophages by ≈60-75% and also decreased E. coli induced oxidative burst in macrophages cells.
Taken together our data indicate that the antioxidants increased severity of peritonitis via decreasing the phagocytic efficiency, oxidative burst, TNF- alpha production and increasing neutrophil infiltration.
Based on these results we propose that antioxidant supplementation during the course of bacterial infection is not recommended as it could be detrimental for the host. Besides, the present study underlines the importance of timing and context of antioxidants administration as opposed to indiscriminate usage to gain best possible therapeutic advantage of these redox compounds.
^
Survival, body weight and peritoneal bacterial load after antioxidant administration in peritonitic mice. (a) Survival of the mice given different treatments over a period of 30 days. The mice were challenged with ~3108 E. coli cells and 500 mg (kg body weight)”1 of one of the antioxidants (GSH/Asc[ascorbic acid]/NAC) through the i.p. route (n56 mice per group). (b) Changes in body weight of the mice during 30 days after injection of E. coli and one of the antioxidants (n56 mice per group). Each data point represents mean±SEM. (c) Changes in peritoneal bacterial load of mice subjected to different combinations of E. coli and antioxidant treatments (n54 mice per group). *P,0.05 compared with the control; #P,0.05 compared with the E. coli-treated group.
Effect of antioxidants on intracellular ROS levels in peritoneal macrophages in vitro
Upon exposure to bacteria, phagocytes produce high levels of ROS by a process called oxidative burst. The bacteria induced alterations in intracellular ROS levels of murine peritoneal macrophages were measured in the presence or absence of exogenously added antioxidants.
...
The decrease in E. coli-induced ROS production was more prominent in macrophages co-incubated with antioxidants compared with those pre-incubated with antioxidants.
...
The present study conceivably proposes that antioxidant administration in animals with bacterial infection could be harmful for the host physiology. This statement is supported by our data that antioxidant administration caused increased bacterial load in the peritonitic mice, ultimately leading to their decreased survival
...
Thus, the antioxidant-mediated decrease in phagocytosis and oxidative burst would disarm the host immune response and thus contribute to the increased bacterial load, leading to higher host mortality. Our proposal is further supported by an independent recent report showing a curcumin-mediated compromised immunological response against invading pathogens in a murine typhoid model (Marathe et al., 2013).
...
Similarly, increased progression of Chlamydia trachomatis infection in the presence of GSH and NAC has been reported previously (Lazarev et al., 2010). Moreover, the presence of supplementary antioxidants at the site of infection could also interfere with the antibody-mediated bacterial killing via the ozonolysis pathway, thereby inhibiting the formation of neutrophil extracellular traps, which facilitate the clearance of bacterial infection from the host’s body (Brinkmann et al., 2004). However, these propositions are yet to be validated experimentally.
...
On the whole, the results of our present study reveal for the first time that antioxidant administration in animals having acute bacterial peritonitis leads to overall deterioration of host conditions. This is the fallout of antioxidant-mediated modulation of three important immunological parameters involved in antibacterial defence:
(i) phagocytic efficacy and oxidative burst;
(ii) neutrophil infiltration and Gr1 expression;
(iii) expression of CD11b, which is a component of complement receptor CR3.
This is an initial but significant step towards understanding the in vivo role of antioxidant supplementation during clearance of bacterial infection. Importantly, we previously established that antioxidants eliminate antibiotic-induced bacterial killing (Goswami et al., 2006, 2007), and our current study indicates that they can also promote bacterial infection by decreasing the capacity of immune cells. Therefore, the knowledge obtained from our previous and present studies strengthens the hypothesis that antioxidants may interfere with the overall clearance of bacterial infections in vivo.
")