Maybe you're not at liberty to discuss, but I'm curious how you're able to obtain it. After researching it for a while, I don't see any other realistic way to increase BH4 other than Kuvan, but my understanding was that it's only available with prescription for a very specific indication now.
@kangaSue 's links explain how.
The key for me was my high phenylalanine on the plasma amino test after taking tyrosine. I also have GCH1 mutations as described by
@SWAlexander which are pretty common and QDPR. These genes have the effect of mild PKU. The effect of the different genes is explained here - note this is not the PKU page which is related to PAH mutations.
https://rarediseases.org/rare-diseases/tetrahydrobiopterin-deficiency/
BioMarin has a team that can help with insurance approvals. I think the price has come down with the generic competition.
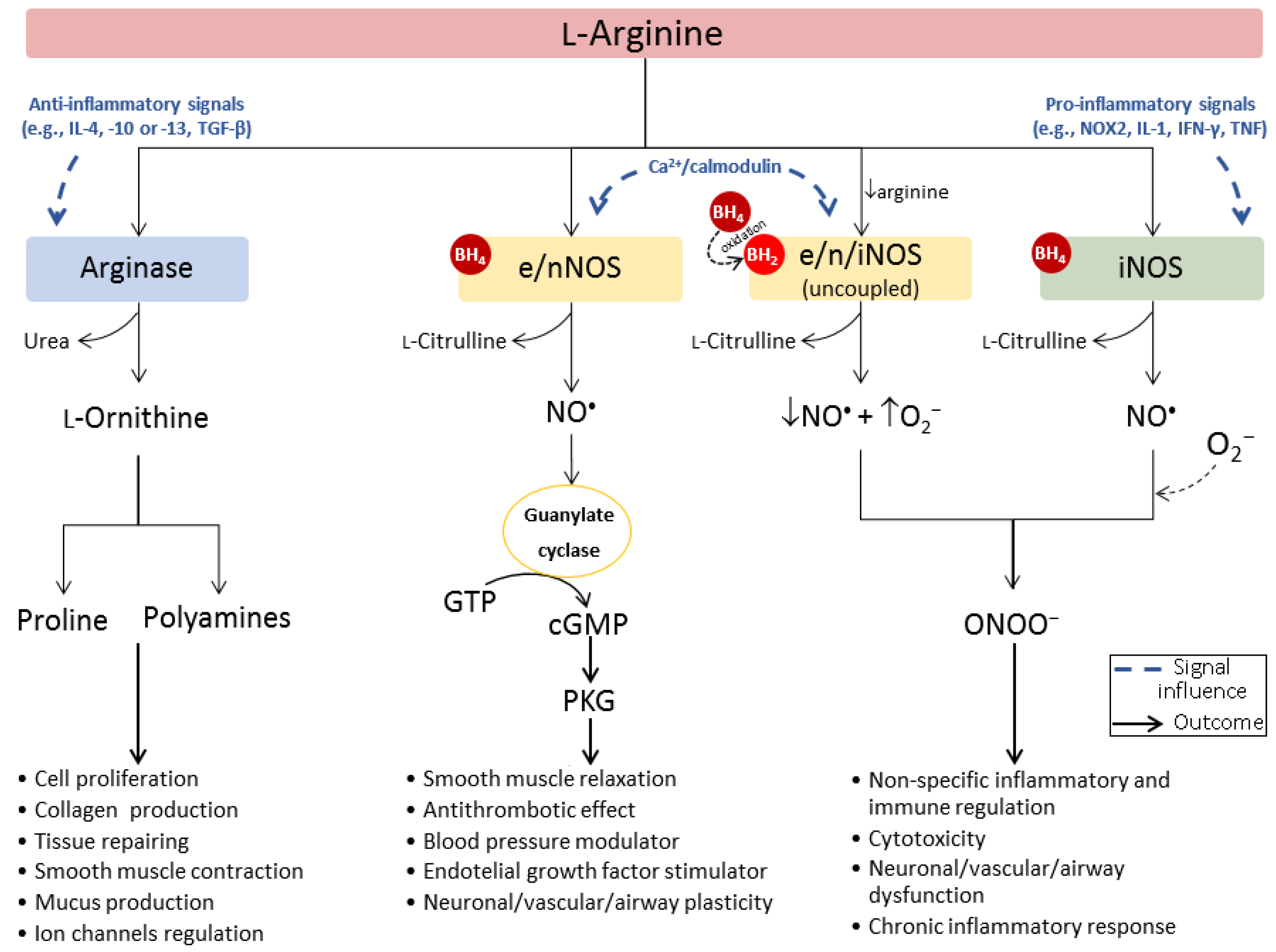
Do you have any references that provide evidence of this? I spent several hours reviewing the literature for my post after the one you replied to, and I can find only a single study that measured NO directly in ME, while all the rest are looking at metabolites, synthase activity, or indirect measures, but all of which seem to support an increase in iNOS activity. I'm willing to believe NO itself could be depleted in ME, I just would like to see any direct evidence that might exist. It seems pretty obvious that iNOS should be upregulated in ME (and one study supports that), but I'd really like to see support for the notion that NO availability in vivo is then abnormal due to this.
I had originally read through as many Pall articles as possible as well as the Morris and Maes oxidative and nitrosative stress article I've posted on several occasions. NO test strips showed I was short of NO and using NO boosters has markedly helped symptoms and reduced my high BP a bit.
Are you not worried about doing further damage by increasing toxic NO metabolites by doing this, or do you feel you can offset that with other things (the supplements Pall advocates for example, as you mentioned)?
I was at first, but there seems to be an inverse relationship between NO and ONOO-. I believe I reacted well to BH4 because I was already using the other supplements Pall suggested.
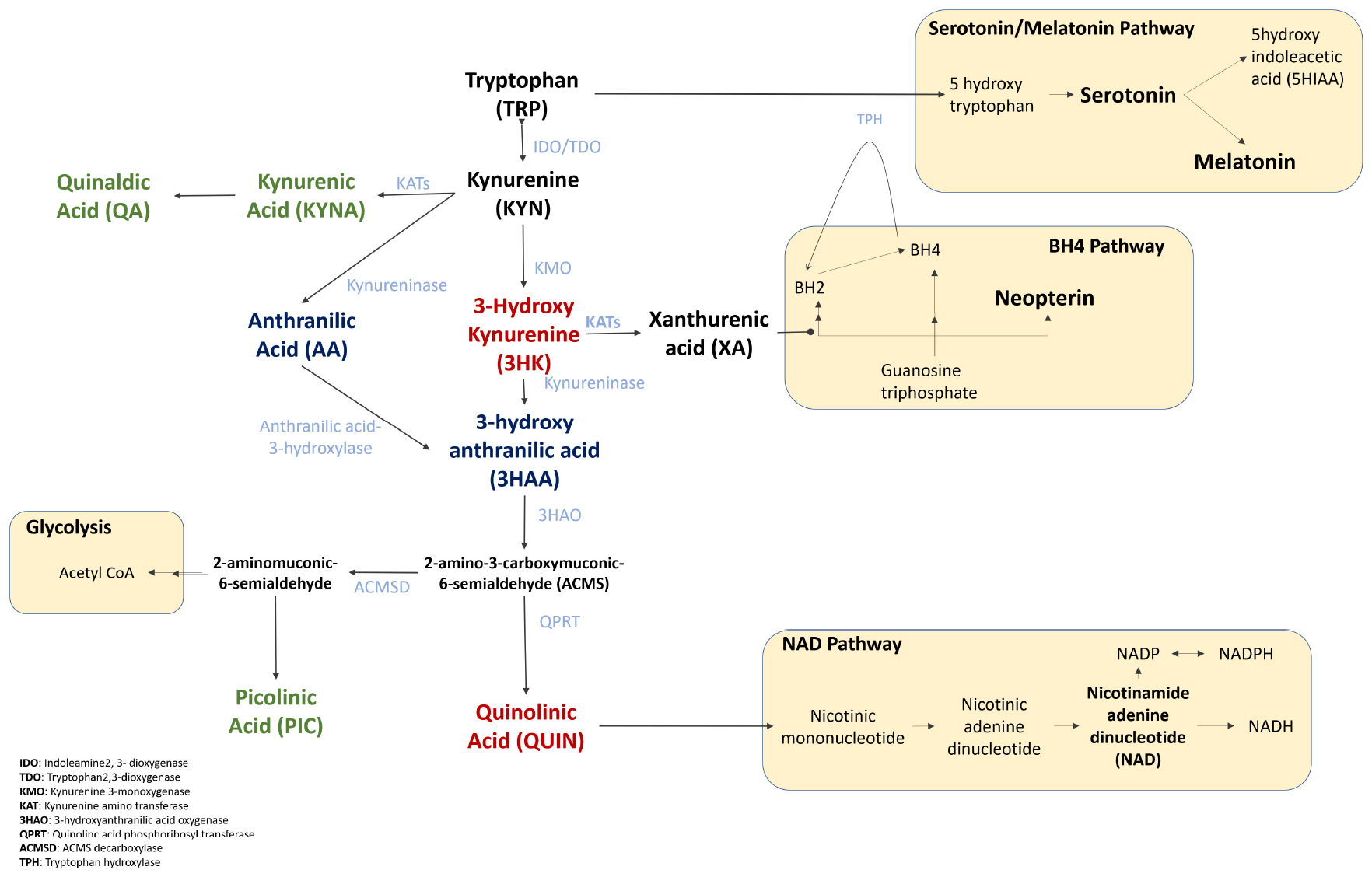
I think the evidence supports this), but at the same time doing so also provides more raw material for kynurenine synthesis and so could increase the amount of neurotoxic kynurenine metabolites if a person didn't do anything else to prevent that (and I still cannot fathom how OMF arrived at the idea of giving people l-kynurenine as a treatment).
I think the key thing is that B6 gets depleted. It's used in over 100 reactions and is critical for several things important for ME/CFS patients, including sphingolipids, oxalate depletion, methylation, heme production, etc.
I would also be interested in which dosage of BH4 Kuvan has helped you @Learner1
I started at 10mg but eventually found I was crashing at 2pm, so went to 20mg which has had a sustainable effect for 2 years. So, I'm using 1 100mg powder packet every 5 days, or 18 every 90 days.
I'm especially interested in CNSA-001 (Sepiapterin) as it is a cheaper alternative
Really? Doesn't look cheaper to me. What's the multiplier between sapropterin and sepiapterin?
Sepiapterin Administration Raises Tissue BH4 Levels More Efficiently Than BH4 Supplement in Normal Mice
Looks like a moneymaker for some pharmaceutical company...

http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2699614/ reports median plasma BH4 levels in patients with this genotype were reduced by approximately 80%. Several potentially serious health issues could result from an 80% reduction in BH4 levels.
There may not be enough BH4 to convert phenylalanine to tyrosine. Therefore, phenylalanine can build up in body tissue and cause health issues (like high blood pressure
Correct. I was chronically a little low in dopamine. My ND had me take 6g of tyrosine daily after I reported being so lethargic I couldn't talk myself into getting off the sofa. That perked me up. That's when I had phenylalanine show up high on the plasma amino acids, as because I was supplementing tyrosine, it backed up.
Additionally, there will be lower available tyrosine, which is needed to create dopamine. Therefore there may not be enough dopamine, which can possibly lead to symptoms similar to conditions like Fibromyalgia and Parkinson’s (but not actually Parkinson’s). People who have low levels of tyrosine, and dopamine, sometimes take a supplement called L-tyrosine, which may help the body to produce enough dopamine to alleviate symptoms and feel better. Instead of L-tyrosine, a doctor may prescribe Levadopa, a prescription of l-dopa, to restore dopamine levels. Extracts of Mucuna pruriens, or velvet bean, can be purchased as an herbal supplement with up to 99% pure l-dopa.
http://www.livestrong.com/article/25194-symptoms-low-dopamine-levels
Correct. Interestingly, my mom had a non-dementia form of Parkinson's for 18 years. Another thing about Parkinson's is impaired mito complex 1, which can happen due to peroxynitrites.