ivorin
Senior Member
- Messages
- 152
So the Ritux results may be out in the next few weeks? Is this just for the trial patients themselves? Sorry to be bothersome, but it's a huge thing for us.Jo Cambridge - Uni College London
Prof of Immunology. Works with Jonathan Edwards
Co-operates with Norwegian team
What B cells are doing in ME/CFS. Results of Norway. Big results should be out in next few weeks
How to possibly identify patients who could benefit from Rituximab treatment?
ME is being recognized as a physical disease now, people in my department in the UK will not agree with me but at least we are here
Virtually ever patient we have studied relates to a viral or inoculation onset
Signalling pathway in stress
Need something that perpetuates the chronic disease. Need something that is hard wired and keeps come back.
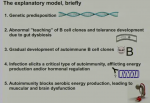
3 steps
Any kind of insult will cause a damage / danger signal
When the infection takes hold the immune system steps in
Memory immune response - B cells make antibodies
Innate immune system - killing of virus infected cells - NK cells - initial response in ME/CFS could be where things start to go wrong
NK cells results published in ME - could be antibody or soluble factors
Cytokines profiles - can tell you what the stimulus is and what the effects will be in lots of tissues
In ME/CFS different cohorts - some cytokines up and down. Decent control cohorts - look at PWME after EBV. Disease duration. Adolescent patients
B cells - inconsistent data. Some say more /less etc.
What did strike us when we reviewed the data was the B-cell viruses were involved in onset for many patients. Onset of B-cell Lymphoma.
Some of the Cytokines reported raised in ME/CFS are related to B-cells
Rituximab used for 20 years in RA and 10 years in Lymphoma. Brave Norwegians she calls them. Rituximab used in 8/10 different diseases in her unit?
Ethical approval could be hard to get as it is a IV infusion - has been said to her. In her own patients not much in the way of problems with reactions. They currently do a test to see if B cells are killed.
Peripheral B cells come out of bone marrow. New naive B cells, most die but some are selected and turn into memory cells or plasma cells. Rituximab doesn't kill stem cells and pro-B cells. Rituximab using immune system to kill B cells. They coat cells and the macrophages kills them.
In tissues B cells are resistant to being killed.
Rituximab is given in large quantities 1-2 grams and coats the B cells in the bone marrow and stops them coming out plus kills the peripheral cells.
Summary of data so far (running through existing research)
£2000 pounds a go for Rituximab in the UK. The blood levels of Rituximab in the Norway studies was huge. She thinks they used a lot of the drug.
She talks about RA in the UK - there are seropositive and seronegative patients. They only use seropositive patients. Showed a slide of all the different condition they treat and the antibody tested
IResponse to Ritaximab epends on how quickly the autoantibody cells regenrate - precusors of autoantibdies
A lot of patients are being treated off label and they haven't responded but it takes a while. She thinks it is a soluble factor or something subtle rather than just the B cells themselves.
Maybe stopping the B cells interacting with other immune cells that could be happening.
If Rituximab works we need to look at B cells.
When the B cells comes back they come back from the naive and the interesting things is that when they B cells relapse is it bad B cells or the number? It's the quality and not the number
Graph of patient in Norway - during period of getting better there were no B cells in the blood. When B cells removed get rid of all the ones turning into memory cells. When they come back (maturing) the ME symptoms came back.
This helps them to work out how to give a dose to stop patients relapsing
Some B cells trigger a relaspe when they come back but some Norway patients are still fine. That suggests that the B cells need to do soemthing to activate again.
Metabolism - B cells sensitive to metabolic activity. How they interact with other cells / pro-inflammatory etc. T cells boring.
B cells can maybe give us indication of what could be happening in our cells. 2 years ago with Fane looked at extended phenotype analysis. 20/30 patients.
No differences in subsets with controls. Then looked at something else - major differences. Subtle. Overlapping populations of B cells. CD24 higher in ME B cells and more molecules per cell. Importnat molecule in B cell maturation. 2 difference in EBV response. AMPK is a key producer. ATP levels. This is related to CD24 and they don't know if the pathway is functioning in ME patients.
Talks about IGM antibodies to EBV
EBV response may be disturbed
B cells have different energy requirements depending on stimulus.
Graph on products between T and non-T dependent responses - lactic acid higher on one
Question - do any of these ME patients have IGM rheumatoid factor or CCP antibodies ?
Answer - in Norway a few IGM but low titres and UK no CCP antibodies