No.
In the context of ICD-11 (which is the context she used the term in) she was correct to use the (proposed but not yet approved) term,
"Bodily
Stress Syndrome".
But this needs qualification and caution, so please read on:
At the moment, in the UK, the following terms are in use:
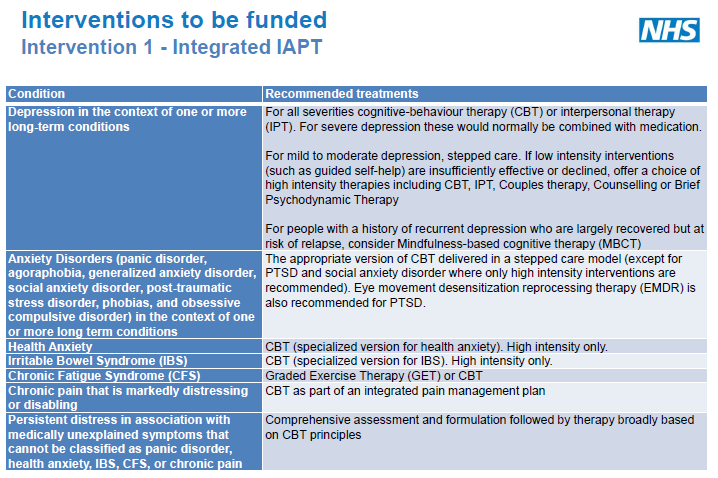
"medically unexplained symptoms" (MUS)
"medically unexplained physical symptoms" (MUPS)
"functional somatic symptoms and syndromes" (FSS)
more recently,
"persistent physical symptoms" (PPS) (as we've seen in this thread, this is increasingly being used in NHS services)
"Bodily Distress Syndrome" (BDS)
"bodily distress disorder" (BDD)
"Bodily distress disorder" is often seen being used interchangeably with "Bodily Distress Syndrome" (BDS) - which is the already operationalized construct and criteria set developed by Fink and colleagues.
The new DSM-5 term "Somatic symptom disorder" (SSD) is also occasionally seen in the UK. SSD has a specific criteria set that is the intellectual property of the APA's publishing arm.
There are two editions of ICD-10:
the ICD-10 "core version" (which can be viewed online)
and
the abridged version of ICD-10's
Chapter 5 Mental and behavioural disorders which is known as
ICD-10 PHC (ICD-10 Primary Health Care). It is used in some countries in primary care and low resource settings.
This has only around 24 disorder categories - the "commonest mental disorders encountered in general medical settings".
The disorder category used in the
ICD-10 PHC primary care version is
"Medically unexplained symptoms."
Whereas, the
ICD-10 core edition has a number of discretely coded somatoform disorder categories (the F45.x categories).
Both the ICD-10 core edition and the abridged Primary Care version are under revision.
Recommendations of external ICD-11 work groups are advisory. Final decisions are made by the ICD-11 Joint Task Force and classification experts and they can override the proposals of the working groups.
Final decisions for ICD-11 have not yet been made.
The revision of the ICD-11 Primary Care version is being led by a working group chaired by Prof David Goldberg (the PCCG group).
The Goldberg group's recommendation is that the existing ICD-10 Primary Care version category "Medically unexplained symptoms" is replaced with a disorder construct which the group proposes to call
"Bodily
Stress Syndrome"
(Which is the term that Prof Payne was struggling with.)
This is a disorder construct that draws heavily on the Fink et al (2010) BDS construct and criteria. It is an adaptation of BDS and is not identical to BDS.
It has not been approved by the ICD-11 Revision Steering Group and Joint Task Force and the group's proposals are evolving. It's been under field testing and is still being evaluated.
(As I've pointed out to Prof Helen Payne, in the comments to her YouTube, it has not been approved for use.)
The Goldberg group proposes that its proposed category "Bodily
Stress Syndrome" would sit under a disorder section heading called "Bodily distress disorders", under which would also sit the category "Health anxiety disorder" or "Illness anxiety disorder."
Like this:
Bodily distress disorders
Code XX Bodily
stress syndrome (replaces Medically unexplained symptoms)
Code XX Health anxiety or Illness anxiety disorder (replaces Hypochondriasis)
So this is a recommendation for the Primary Care version by an external working group which is still evolving and which has not been approved and which may be rejected.
There is expected to be alignment between disorder categories in the ICD-11 core edition and the 28 mental health disorders to be included in the forthcoming ICD-11 Primary Care version.
For the
ICD-11 core edition, the recommendations for the revision of the various F45.x somatoform disorder categories are the responsibility of the
S3DWG sub working group. This group is chaired by Prof Oye Gureje. Prof Francis Creed is also a member.
So we have two largely autonomous working groups making divergent recommendations for revision of the ICD-10 somatoform disorder categories.
The
S3DWG's recommendation (
which has been entered into the core version Beta draft) is for a disorder construct which they currently propose to call
"Bodily distress disorder" (BDD)
This single category with three severities (Mild, Moderate, Severe) would replace most of the ICD-10 Somatoform disorder categories and also subsume F48 Neurasthenia, which is proposed to be retired for ICD-11 for both the core and the primary care versions.
However, in construct, definition, characteristics and criteria, ICD-11's BDD is closely aligned to DSM-5's "Somatic symptom disorder". "Somatic symptom disorder" has also been listed under "Synonyms" to BDD.
Fink's BDS does not appear in the ICD-11 core edition Beta draft and there are reasons which would make it problematic to locate under BDS under the Mental and behavioural chapter. For example, BDS requires no psychobehavioural cognitions (psychological criteria) to meet the criteria.
(Fink has said that he tried to get ICD-11 to create a special section under which BDS might be located, but this has been unsuccessful.)
SSD and Fink's BDS are conceptually different, with different criteria sets and they potentially capture different patient populations (which both DSM-5's Dimsdale and Fink acknowledge).
SSD and ICD-11's proposed BDD can be applied to patients with symptoms associated with general medical conditions, which Fink's BDS and the Primary Care group's proposed BSS can't.
To sum up:
Recommendation by the S3DWG for ICD-11 core edition -
Bodily distress disorder (close to SSD).
Recommendation by the PCCG for ICD-11 Primary Care version -
Bodily stress syndrome (close to BDS).
But as I've said above, the term "BDD" is already being used interchangeably in the field for the operationalized "BDS".
So there is considerable potential for confusion between these various terms.
Unless you have read the proposal papers and scrutinized the definitions, characterizations and criteria and proposed definitions and criteria, it can be difficult to understand the differences between them.
Leaving aside the issue of lack of validity for
any of these constructs, proposing to introduce a new disorder term in the next edition of ICD-11, the proposed name for which is already closely associated with a conceptually divergent disorder construct, will potentially lead to conflation between the ICD-11 BDD construct and the Fink BDS construct with implications for maintaining construct integrity.
(Which is possibly what Prof Creed would embrace, since he is known not to favour the SSD construct, himself.)
The issue of nomenclature has been under discussion with ICD Revision for several years and whilst acknowledged as problematic by ICD-11's Dr Geoffrey Reed, with whom I am in contact, it remains unresolved.
There are reasons why ICD Revision won't use the SSD term and construct instead of its proposed BDD, which I don't have time this morning to go into.
So back to your question: yes, Prof Payne
was correct to use the term "Bodily
stress syndrome" in the context of ICD-11.
However, she failed to clarify:
1) that the BSS proposal is from the abridged Primary Care version work group;
2) that BSS has not been approved for the Primary Care version or the core edition;
3) that a different disorder construct and criteria set is under consideration from the S3DWG group and it is this alternative proposal (currently named BDD) that has been entered into the ICD-11 core Beta draft.
It's complicated, I know