
I have AMP deaminase deficiency (genetic). My endurance sucked all my life, and my recovery time from exercise was always longer, even as a child, but I never had PEM or any other ME symptoms. I guess if things had gone differently this common genetic disorder would have been completely unimportant, but in light of my illness I wonder if exploring AMP metabolism might be worthwhile. Sorry to dump on your thread Hip but I was wondering if you think there is a "best" metabolic test out there at the moment that would cover many of the bases surrounding AMP metabolism.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Mitochondrial and Energy Metabolism Dysfunction in ME/CFS — Myhill, Booth and McLaren-Howard Papers
- Thread starter Hip
- Start date
Hip
Senior Member
- Messages
- 18,313
So Mary's MES score is just 11% of a normally healthy person's score.
Yes just 11% of normal (or even less, because as you can see from the graph, the MES value that healthy people have starts at 1, and goes up to around 2).
Last edited:
realturbo
Senior Member
- Messages
- 143
@Hip I'm amazed that you are able/willing to provide such detailed and clear responses - not sure how you do it, and how long it takes you to write up such comprehensive replies. I salute you for the effort and time you put into sharing your knowledge with others!@Mary Looking at your ATP Profiles test results, the five decimal figures .......
Hip
Senior Member
- Messages
- 18,313
Thank you, @realturbo, though it's partly because I have reading difficulties, ADHD as well as brain fog, so I find I need to write posts slowly and methodically. But anyway, I have always enjoyed trying to explain technical subjects in a (hopefully) easy to grasp language.
Mary
Moderator Resource
- Messages
- 18,339
- Location
- Texas Hill Country
@Hip - thanks for your follow-up post, I've just skimmed it briefly. I had to do some errands and am a bit sick so will not get to peruse anything in depth for a day or 2 (or 3) - but again I appreciate it so much, your analysis looks very interesting! ")
Mary
Moderator Resource
- Messages
- 18,339
- Location
- Texas Hill Country
Hi @Hip - well, I got to this more quickly than I thought I would be able to. All I can say is wow - seeing the graph with my name near the bottom brought it home to me in a very real way how severe my ME/CFS is. I’ve long thought I had "moderate" ME/CFS, because I don’t have brain fog, I don’t have pain, I don’t have severe OI (though I do have moderate OI or POTS [not sure which! Or they may be the same?]).
But my energy production is severely curtailed and I crash regularly if I am not very very careful (which I try to be of course), and I get sick every time I crash, without fail. (And sick in between too ...), and my NK function is quite low too.
In going through your posts to me, I ended up going through your initial post re Myhill, McLaren et al., line by line (which I had not done before) and it was fascinating. I’d seen Myhill’s explanation of PEM before, which I thought was rather elegant, but I’d never seen the categories of patients into groups A and B and never really tried to grasp before what the heck was going on with our ATP. You’ve managed to explain some rather complex concepts in a very well organized, comprehensible form - you’ve done us all a great service!
It’s very helpful to me that you pointed out my chief problems with energy production are ADP to ATP conversion, and oxidative phosphorylation. Based on your recommendation, I am increasing my daily d-ribose from 5 mg to 15. Several years ago I was taking 10 mg. a day and then cut back, partly trying to save money, partly thinking I’ve been taking it for so long, I must not need it as much any more - but I think I was wrong on both counts (and of course it was a false economy. I’m also going to try taking extra when I’m crashed and see what happens.
Re oxidative phosphorylation and CoQ10 - I did try increasing my CoQ10 intake recently from 400 mg a day to 600 or 700 mg while crashed, and ended up wired but severely fatigued at the same time. And then I figured out that the increased CoQ10 (which I should have increased gradually!) caused my phosphate to tank. Another supplement did this to me before, can’t remember which one right now, but that’s when I first identified fatigue resulting from phosphate depletion. In reading about refeeding syndrome, I discovered the hallmark of refeeding syndrome is hypophosphatemia.
So then I read in your post that oxidative phosphorylation involves recycling ADP to ATP, by adding phosphate to ADP. Which could explain how my phosphate tanked when taking the extra CoQ10. It all made sense. Whew! So I am going to try increasing my CoQ10 again, gradually, but also while keeping a close eye on phosphate levels.
I also found your theory re coxsackievirus B (which I have), autoimmunity and translocator protein very interesting. Your recommendation of a drug or supplement which could affect the cell membrane in order to block the autoantibodies from getting into the cell made me think of NT Factor which is supposed to repair cell membranes. A few years ago I was given a free supply of NT Factor (it’s pretty pricey) but unfortunately it did nothing for me, though I think it may be helpful to some others. It doesn’t mean your theory is incorrect, of course - there are so many variables involved.
One other thing came to mind - I was wondering if there was any correlation between Coxsackie B - induced myocarditis, and abnormal impedance cardiography results. I had a full heart work up 5 years ago or so, and everything was great (despite, at that time, no exercise for over 12 years!). But an impedance cardiography done some 9 years ago showed significant abnormalities. I’m sure you’ve seen Andrew Peckerman’s paper correlating abnormal impedance cardiography results with severity of ME/CFS symptoms: https://www.ncbi.nlm.nih.gov/pubmed/12920435
However, I don’t have symptoms of myocarditis so there may be no connection here apart from cardiac abnormalities in both instances.
Anyways, thanks again for all your help - I am so glad you enjoy explaining technical subjects to the rest of us!
But my energy production is severely curtailed and I crash regularly if I am not very very careful (which I try to be of course), and I get sick every time I crash, without fail. (And sick in between too ...), and my NK function is quite low too.
In going through your posts to me, I ended up going through your initial post re Myhill, McLaren et al., line by line (which I had not done before) and it was fascinating. I’d seen Myhill’s explanation of PEM before, which I thought was rather elegant, but I’d never seen the categories of patients into groups A and B and never really tried to grasp before what the heck was going on with our ATP. You’ve managed to explain some rather complex concepts in a very well organized, comprehensible form - you’ve done us all a great service!
It’s very helpful to me that you pointed out my chief problems with energy production are ADP to ATP conversion, and oxidative phosphorylation. Based on your recommendation, I am increasing my daily d-ribose from 5 mg to 15. Several years ago I was taking 10 mg. a day and then cut back, partly trying to save money, partly thinking I’ve been taking it for so long, I must not need it as much any more - but I think I was wrong on both counts (and of course it was a false economy. I’m also going to try taking extra when I’m crashed and see what happens.
Re oxidative phosphorylation and CoQ10 - I did try increasing my CoQ10 intake recently from 400 mg a day to 600 or 700 mg while crashed, and ended up wired but severely fatigued at the same time. And then I figured out that the increased CoQ10 (which I should have increased gradually!) caused my phosphate to tank. Another supplement did this to me before, can’t remember which one right now, but that’s when I first identified fatigue resulting from phosphate depletion. In reading about refeeding syndrome, I discovered the hallmark of refeeding syndrome is hypophosphatemia.
So then I read in your post that oxidative phosphorylation involves recycling ADP to ATP, by adding phosphate to ADP. Which could explain how my phosphate tanked when taking the extra CoQ10. It all made sense. Whew! So I am going to try increasing my CoQ10 again, gradually, but also while keeping a close eye on phosphate levels.
I also found your theory re coxsackievirus B (which I have), autoimmunity and translocator protein very interesting. Your recommendation of a drug or supplement which could affect the cell membrane in order to block the autoantibodies from getting into the cell made me think of NT Factor which is supposed to repair cell membranes. A few years ago I was given a free supply of NT Factor (it’s pretty pricey) but unfortunately it did nothing for me, though I think it may be helpful to some others. It doesn’t mean your theory is incorrect, of course - there are so many variables involved.
One other thing came to mind - I was wondering if there was any correlation between Coxsackie B - induced myocarditis, and abnormal impedance cardiography results. I had a full heart work up 5 years ago or so, and everything was great (despite, at that time, no exercise for over 12 years!). But an impedance cardiography done some 9 years ago showed significant abnormalities. I’m sure you’ve seen Andrew Peckerman’s paper correlating abnormal impedance cardiography results with severity of ME/CFS symptoms: https://www.ncbi.nlm.nih.gov/pubmed/12920435
However, I don’t have symptoms of myocarditis so there may be no connection here apart from cardiac abnormalities in both instances.
Anyways, thanks again for all your help - I am so glad you enjoy explaining technical subjects to the rest of us!
- Messages
- 33
any other mitochondria test out there besides Myhill's?
Hip
Senior Member
- Messages
- 18,313
I’ve long thought I had "moderate" ME/CFS, because I don’t have brain fog, I don’t have pain, I don’t have severe OI (though I do have moderate OI or POTS [not sure which! Or they may be the same?]).
But my energy production is severely curtailed and I crash regularly if I am not very very careful (which I try to be of course), and I get sick every time I crash, without fail. (And sick in between too ...), and my NK function is quite low too.
That is very interesting, because when I was contemplating the Myhill, Booth and McLaren-Howard theory of energy metabolism dysfunction in ME/CFS, my thoughts were that a defective energy metabolism could well be the central pathophysiology in ME/CFS, but that there might also be other pathophysiologies simultaneously going on in ME/CFS, such as low level chronic enteroviral brain infection (perhaps a cause of brain fog), chronic viral muscle infections (perhaps a cause of muscle inflammation and muscle pain), or virally-triggered autoantibodies (perhaps a cause of POTS or orthostatic hypotension).
So maybe these other symptoms of brain fog, pain, or orthostatic intolerance symptoms do not necessarily stem from just the energy metabolism dysfunction, but arise from viral infection/autoimmunity (but perhaps are worsened by the energy shortage).
You’ve managed to explain some rather complex concepts in a very well organized, comprehensible form - you’ve done us all a great service!
Pleased that you found it useful. But I think the credit has to go to Myhill, Booth and McLaren-Howard for developing such an incisive theory of ME/CFS. I don't know why this theory did not get the attention it deserved when it was first published in 2009. It will be very interesting, as new study results come in (such as Fluge and Mella's current in-depth investigations into ME/CFS metabolism), to see how the latest ME/CFS metabolic findings fit in with Myhill et al's original theory of ME/CFS energy metabolism dysfunction.
I am increasing my daily d-ribose from 5 mg to 15. Several years ago I was taking 10 mg. a day and then cut back, partly trying to save money, partly thinking I’ve been taking it for so long, I must not need it as much any more - but I think I was wrong on both counts (and of course it was a false economy. I’m also going to try taking extra when I’m crashed and see what happens.
After reading the Myhill, Booth and McLaren-Howard theory of PEM, my hunch is that increased D-ribose may be particularly helpful at times of increased energy expenditure and when PEM subsequently appears, because their theory states that PEM results when you have actually physically lost a large amount of your ATP/ADP molecules, as these molecules get broken down and are flushed out of the body in the urine. Normally the ATP/ADP molecules are constantly recycled by oxidative phosphorylation in the mitochondria, so you don't normally lose them.
Thus during PEM, D-ribose should in theory be particularly helpful, as D-ribose can be used to manufacture some brand new ATP molecules (by de novo synthesis of ATP), which are desperately needed during PEM.
By the way, there are some good prices for bulk D-ribose powder on PureBulk.com and on BulkSupplements.com.
So then I read in your post that oxidative phosphorylation involves recycling ADP to ATP, by adding phosphate to ADP. Which could explain how my phosphate tanked when taking the extra CoQ10. It all made sense. Whew! So I am going to try increasing my CoQ10 again, gradually, but also while keeping a close eye on phosphate levels.
Interesting thought! That is certainly worth exploring. The Myhill et al papers do talk about a possible shortage of inorganic phosphate (Pi) in some ME/CFS patients, but I believe this tends to be the Group A2 patients (who Myhill et al say may also have a shortage of Krebs cycle substrates, as well as Q10, NADH and magnesium shortages — see Myhill 2012).
You are definitely not a Group A2 patient though, because to be Group A2 patient you first of all have to have oxidative phosphorylation running normally (and yours is running under par), and secondly you need to have higher than normal (super-normal) values of Translocator Protein In (whereas you have a low value of 0.25). Just a reminder that the patient groups are detailed in this earlier post.
It might be an idea though to try taking some phosphate / phosphorous supplements with your Q10, to see if that helps.
Your recommendation of a drug or supplement which could affect the cell membrane in order to block the autoantibodies from getting into the cell made me think of NT Factor which is supposed to repair cell membranes.
Yes, the NT Factor is supposed to affect the cell membrane. So is the VegEPA® supplement that Professor Bassant Puri's studies found was helpful for ME/CFS in some patients — I have some VegEPA on my shelf to try, but have not got around to trying it yet.
By the way, the finding in your Mitochondrial Translocator Protein Study of lanolin potentially blocking your translocator protein may be worth following up on. Lanolin gunking up your translocator protein could in part explain your low Translocator Protein In value of 0.25.
My understanding is that when the substances blocking the translocator protein are addressed, this can lead to improvements in ME/CFS symptoms.
The lanolin potentially blocking your translocator protein would, I think, probably come from cosmetics such as skin moisturizers. So you could try switching to lanolin-free products, and seeing if that helps.
One further point: I think I have figured out what the "15/100" figure that Dr Myhill wrote at the bottom of your ATP Profiles test results mean: I believe this 15% figure refers to where you are calculated to be on the Bell CFS Disability Scale, given the MES value of 0.11 that you have.
The 15% figure can be determined by looking at where your MES value of 0.11 (the purple line) intersects the diagonal dotted line in the figure below (the same figure that I posted earlier), which you can see is around 1.5 (= 15%) on the horizontal axis of the graph:
In this post on another thread, someone else uploaded their ATP Profiles test results, and they had a MES = 0.40, which when you look at where 0.40 intersects the diagonal dotted line, it works out as 4 on the horizontal axis, ie, 40% on the Bell CFS Disability Scale, which is why I believe Dr Myhill has hand written a "40/100" figure at the bottom of the page.
Last edited:
Hip
Senior Member
- Messages
- 18,313
I have AMP deaminase deficiency (genetic). My endurance sucked all my life, and my recovery time from exercise was always longer, even as a child, but I never had PEM or any other ME symptoms.
AMP deaminase deficiency is a new one for me, but according to Wikipedia, AMP deaminase is an enzyme that converts AMP to inosine monophosphate (IMP). Since conversion of AMP to IMP forms part of the pathway by which AMP is flushed from the body, leading to PEM according to the theory (see this post), my first thought is that if you had the usual virally-triggered ME, you might actually be less prone to getting PEM.
Looking at the Wikipedia article, AMP deaminase deficiency seems quite complicated and not very well understood, so it is hard to suggest anything. The article does say that one of the issues is loss of ribose and fumarate, so you might want to try taking D-ribose and fumarate, if you are not already. Also it says that low levels of nitric oxide may be an issue, so some NO boosting supplements like arginine and dietary nitrates (eg beetroot juice) might help.
Hip
Senior Member
- Messages
- 18,313
any other mitochondria test out there besides Myhill's?
I am not aware of any, but I don't know much about mitochondrial and energy metabolism tests.
Indigophoton
Senior Member
- Messages
- 127
- Location
- UK
I had this test done in 2008, when I was considerably less severe than now. I posted the results in another thread
It looks like this -
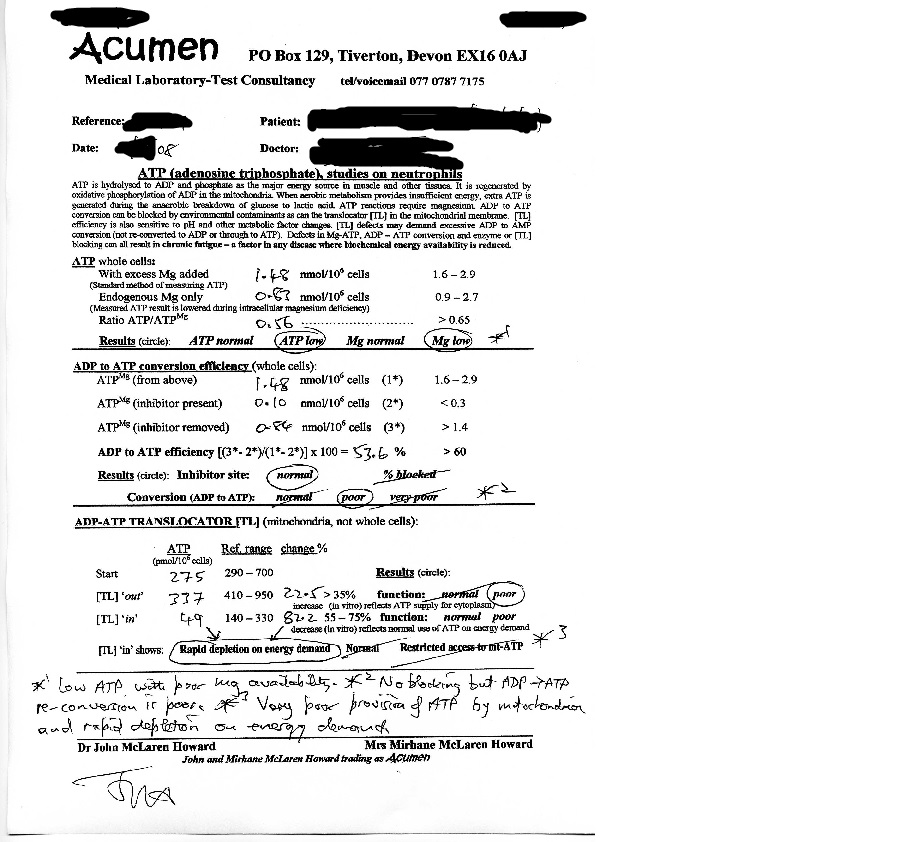
The annotations are by Dr McLaren Howard. Presumably the figures would be worse now, if they accord with severity.
I've got too much brain fog to follow all this at the mo, but would guess I might fall into group B, because I find d-ribose very helpful. At my most severe I couldn't even lift my head off the bed, and every moment was one of just hanging in in considerable discomfort. Based on a sudden intuition one day I upped my d-ribose from 15 to 100g a day, and it was immediately helpful in easing the incredible strain my body was under. After a few months I was back to being able to get to the bathroom.
I still take it five times a day although less (not sure in grams). The only downside at the very high dose was some gastric issues, but the benefits were immense; I was heading for being tube-fed etc and it saved me.
It looks like this -
The annotations are by Dr McLaren Howard. Presumably the figures would be worse now, if they accord with severity.
I've got too much brain fog to follow all this at the mo, but would guess I might fall into group B, because I find d-ribose very helpful. At my most severe I couldn't even lift my head off the bed, and every moment was one of just hanging in in considerable discomfort. Based on a sudden intuition one day I upped my d-ribose from 15 to 100g a day, and it was immediately helpful in easing the incredible strain my body was under. After a few months I was back to being able to get to the bathroom.
I still take it five times a day although less (not sure in grams). The only downside at the very high dose was some gastric issues, but the benefits were immense; I was heading for being tube-fed etc and it saved me.
Mary
Moderator Resource
- Messages
- 18,339
- Location
- Texas Hill Country
So maybe these other symptoms of brain fog, pain, or orthostatic intolerance symptoms do not necessarily stem from just the energy metabolism dysfunction, but arise from viral infection/autoimmunity (but perhaps are worsened by the energy shortage).
I've wondered the same thing. I don't have antibodies to the cytomegalovirus, and I've wondered if this virus is responsible for brain fog or other complications which I don't have. Also my former ME/CFS doctor (who died last May), although he could not do anything for PEM, did have me on a good basic nutritional regimen, including MB12 for many years, even prior to when I started crashing in 1998. So I've wondered if this is a factor too in my lack of brain fog. but I don't know of course.
By the way, there are some good prices for bulk D-ribose powder on PureBulk.com and on BulkSupplements.com.
Thanks! will check them out.
The lanolin potentially blocking your translocator protein would, I think, probably come from cosmetics such as skin moisturizers. So you could try switching to lanolin-free products, and seeing if that helps.
I just checked my face cream and lotions and none of them currently have lanolin - whew! but will keep an eye out for this in the future.
I know the test also mentioned a "diamino compound" - dye precursor (possibly to hair dye) blocking translocator protein. I used to infrequently highlight my hair but never overall hair color and haven't done anything for over a year, so I don't know how much of a factor this is.
However, I just googled "diamino acetone" for the heck of it as I had a job when I was 19 where I had heavy exposure to acetone - we worked with resins making fake Tiffany lamps and used to wash our hands in acetone - we were breathing it all day. It was a fire trap and eventually burned (luckily no one was in it at the time!) but at 19 I thought it was cool to have a job where you got a little bit high from breathing fumes ......
So diamino acetone is a real thing. So I'm guessing that may be the culprit here. I did a liver detox some 13 years ago, my liver was having a really rough time, due in large part to chemical solvents and it has been much better since.
One further point: I think I have figured out what the "15/100" figure that Dr Myhill wrote at the bottom of your ATP Profiles test results mean: I believe this 15% figure refers to where you are calculated to be on the Bell CFS Disability Scale, given the MES value of 0.11 that you have.
Thank you Hip - another mystery solved.
It might be an idea though to try taking some phosphate / phosphorous supplements with your Q10, to see if that helps.
I am going to do this. The fatigue was so bad, I don't want to go through that again. FWIW, I found that kefir is a great source of phosphorous and also Swanson Vitamins sells monosodium phosphate and a very small dose of that in kefir really helps. Also I eat a lot of sunflower seeds now, also high in phosphorous.
Thanks again for all your input --
Hip
Senior Member
- Messages
- 18,313
guess I might fall into group B, because I find d-ribose very helpful.
Yes, I think you are in Group B, because your ADP to ATP Conversion (oxidative phosphorylation) efficiency is described as "poor" in your test results, which puts you in Group B.
Your magnesium is described as "low" too, so magnesium supplementation may help, if you are not taking it already. In the cell, the ATP molecule has to bond onto a magnesium molecule before the ATP can release its energy, so a shortage of magnesium in the cell can reduce energy supply.
Transdermal application of magnesium gets a higher dose of magnesium into the body than oral magnesium (orally you are limited by the bowel flushing / diarrhea that occurs at higher doses). When I have applied magnesium transdermally on my skin from head to toe, I used a very concentrated solution of Epsom salts placed in an old household cleaner spray bottle, for easy application (see this post). Vitamin B6 and B1 are cofactors that promote the absorption of magnesium into cells.
Based on a sudden intuition one day I upped my d-ribose from 15 to 100g a day, and it was immediately helpful in easing the incredible strain my body was under. After a few months I was back to being able to get to the bathroom.
Very interesting. So going beyond Dr Myhill's recommendation of 15 grams of D-ribose daily (taken in divided doses) can bring significant results.
It says here that the gut can absorb around 15 grams of D-ribose per hour (it says the small intestine can absorb "200 mg/kg/h"). So maybe the best dosing would be taking the 100 grams of D-ribose in say 5 divided doses throughout the day, to help avoid gastric issues.
As an aside, did you ever see this post of about the benefits I obtained from high dose selenium (400 mcg of selenomethionine daily on an empty stomach). That is the protocol that I found arrested my slide into severe ME/CFS, and kept me in the moderate category. Selenium is antiviral for coxsackievirus B. This protocol also helped a few others, but some people who tried it found it was too overstimulating.
Hip
Senior Member
- Messages
- 18,313
I had a job when I was 19 where I had heavy exposure to acetone - we worked with resins making fake Tiffany lamps and used to wash our hands in acetone - we were breathing it all day.
I don't think acetone itself would be a problem, because acetone is a part of normal metabolism, and thus the body knows how to handle it (during fasting or calorie restriction, when the body initiates ketosis, acetone is one of the ketone bodies made by the metabolism — in fact, acetone has anticonvulsant properties, and acetone thought to be one of the reasons that a ketogenic diet helps epilepsy).
Mary
Moderator Resource
- Messages
- 18,339
- Location
- Texas Hill Country
I don't think acetone itself would be a problem, because acetone is a part of normal metabolism, and thus the body knows how to handle it (during fasting or calorie restriction, when the body initiates ketosis, acetone is one of the ketone bodies made by the metabolism — in fact, acetone has anticonvulsant properties, and acetone thought to be one of the reasons that a ketogenic diet helps epilepsy).
Well, I think in high enough amounts - and I had heavy exposure, both breathing it for 8 hours a day for 8 or 9 months (cannot remember exactly!) plus washing my hands in it - can cause damage, according to the CDC:
https://www.atsdr.cdc.gov/toxfaqs/tf.asp?id=4&tid=1Health effects from long-term exposures are known mostly from animal studies. Kidney, liver, and nerve damage, increased birth defects, and lowered ability to reproduce (males only) occurred in animals exposed long-term. It is
Hip
Senior Member
- Messages
- 18,313
My understanding is that the translocator protein studies at Acumen Labs are performed in order to detect any substances that are accumulating on the mitochondrial translocator protein, and potentially blocking its functioning.
I wouldn't have thought that acetone can bioaccumulate on translocator protein. It is a volatile substance that when created in the body is exhaled in the breath. It can of course be toxic at certain levels. But it's academic anyway, as acetone was not found during your translocator protein studies.
Note that Myhill et al use the term "translocator protein" to refer to the adenine nucleotide translocator (ANT).
I wouldn't have thought that acetone can bioaccumulate on translocator protein. It is a volatile substance that when created in the body is exhaled in the breath. It can of course be toxic at certain levels. But it's academic anyway, as acetone was not found during your translocator protein studies.
Note that Myhill et al use the term "translocator protein" to refer to the adenine nucleotide translocator (ANT).
Last edited:
Indigophoton
Senior Member
- Messages
- 127
- Location
- UK
Your magnesium is described as "low" too, so magnesium supplementation may help, if you are not taking it already.
Yes, thanks, I need quite a bit of magnesium. I think I'm at the optimal dose: any more and it makes me weak(er) and sleepy. Any less and I start getting chest pains. So it's a fairly easy one to keep in balance.
Very interesting. So going beyond Dr Myhill's recommendation of 15 grams of D-ribose daily (taken in divided doses) can bring significant results.
Yes, it would be interesting to know if anyone else who identifies themselves as being in Group B finds large doses beneficial.
D-ribose is a sugar but curiously enough, even when I was consuming a kilogram every ten days, it did not result in any weight gain.
The other minor side effect I forgot to mention is that it lowers blood sugar temporarily, which I found resulted in light-headedness, so it's best taken with food to prevent that. It dissolves in water very easily.
Interesting, thanks, I take 100mcg seleniomethionine, but I will try it as you suggest once the new medicine I've just started has levelled out.As an aside, did you ever see this post of about the benefits I obtained from high dose selenium
arewenearlythereyet
Senior Member
- Messages
- 1,478
Great to see the mitochondrial aspect being discussed. I stumbled on the myhill site shortly after being diagnosed in 2013. I was sceptical about the content at first since some of the alternative lifestyle stuff seemed a bit extreme/unsubstantiated and I was a little suspicious about the conflict of interest due to the online shop. However the PEM theory seemed to make sense. I gave the d ribose a go and I am now on 10-30g a day. This seemed to drop the severity of the episodes for me. Before taking it I would be laid up for around 3-4 days. Now it's 12-24 hrs recovery time when I over do it. I take 10g in a coffee (decaf) instead of sugar but I guess you could dissolve it in water. Seems to perk me up in the morning so this is now part of my daily ritual. I am in a sort of remission due to pacing mainly and I would say I am a 55 on the bell scale (although my weekends are pants activity wise). I have got my PEM episodes down to once every 2-3 weeks, but as I said these are now mainly just a day lost.
Just my experience mind you
Just my experience mind you
Hip
Senior Member
- Messages
- 18,313
Before taking it I would be laid up for around 3-4 days. Now it's 12-24 hrs recovery time when I over do it.
Wow, that's quite a difference just from taking D-ribose.
arewenearlythereyet
Senior Member
- Messages
- 1,478
Wow, that's quite a difference just from taking D-ribose.
Yes it is possible that because I took it early on in my regime that other things came into play as well (heart rate monitoring pacing etc.). I am however reluctant to stop something that might be working. I look at mitochondrial support as a necessity until I can start methylation properly, so even though it's expensive I need to look after them. After the d ribose seemed to be working I then started taking oral and sub dermal magnesium and a range of other supplements that may also help, but the ribose effect was one of the first supplements that seemed to have an affect. I also now prefer the taste to sugar which in comparison seems overly sweet.