I think they are pretty unambiguous in their analysis of the data.
I actually think they were ambiguous! I heard the story on NPR and the resulting discussion. Both the health reporter who did the story, and you, came away with the conclusion:
Koan said:
Recent studies have shown that commonly prescribed antidepressants are really no better than placebo in relieving depression.
Let's look at the conclusion you bolded. I'm sorry if I'm being over explanatory and redundant! I'm not sure why you bolded it but I'll go ahead and explain what it means:
The findings also show that the effect for these patients seems to be due to decreased responsiveness to placebo, rather than increased responsiveness to medication.
Right. So what this means is that as the more severe the patient, the less effective the placebo. The resposne didn't increase, but it doesn't mean the anti depressant is not effective. (The response actually drops off a bit.)
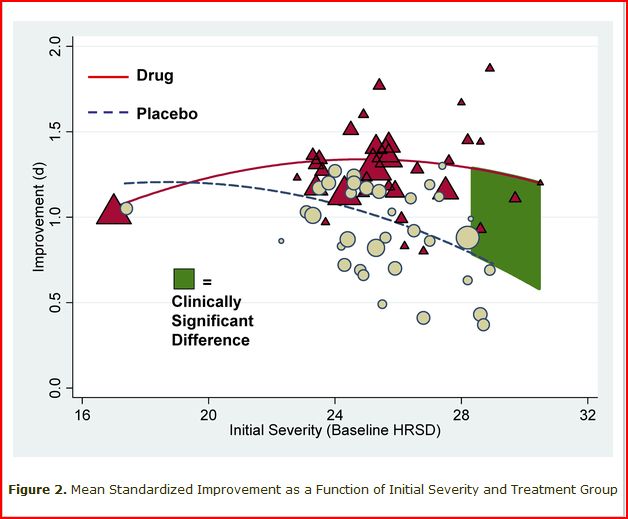
Here's a graph from the study (I embedded it because the link was to a clunky PDF):
So, the bottom part of the graph shows the way the patients were "rated" for depression, based on severity. A score of 19 means the patient is "severe", 23 means they are "very severe", and anything over 28 is the "most severe".
So, clinical significance comes into play when drug works a LOT better than placebo. So, placebos work as well or better up until you get to 20, and then they work better (but not significantly better) than placebo until you get to the very sickest patients, for whom they work very well.
Does it make sense now?
Again, I'm sorry if you already understood it and I'm overdoing the explaining!

Koan said:
In fact, it argues against an easily manipulated mind/body connection as the efficacy of the placebo effect dropped off when it could be said with more certainty that the underlying illness was most likely biologically based.
I wish I knew more about the placebo effect. In the study they mentioned that placebo in pain medication was 50%, which seems really high to me. It would be interesting to see what it is in say, infection, or wound care. I do know that it might be low for CFS patients!
http://www.medscape.com/viewarticle/538172
:tear: