Joint response from the Countess of Mar's Forward-ME group:
(ME Association, ME Research UK, Action for M.E., Tymes Trust, reMEmber CFS, Blue Ribbon Awareness of ME (BRAME), ME Trust, the 25% ME Group, and Invest in ME)
http://apps.who.int/classifications...lGroupId=4b26ab6a-393f-4a39-9051-4ac1d4b1a55a
Forward-ME is a group of UK charities and voluntary organisations convened by the Countess of Mar, in order to promote effective joint working by M.E. and CFS organisations.
The organisations are ME Association, ME Research UK, Action for M.E., Tymes Trust, reMEmber CFS, Blue Ribbon Awareness of ME (BRAME), ME Trust, the 25% ME Group, and Invest in ME.
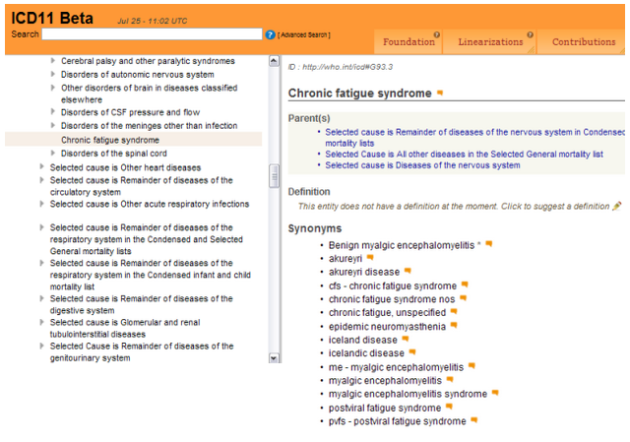
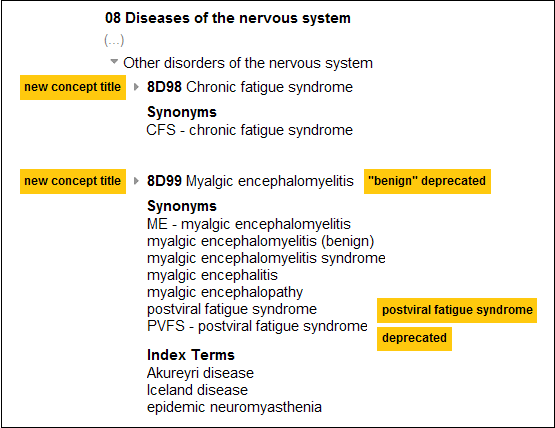
We are in agreement that, as proposed here, it is particularly important for Myalgic encephalomyelitis (M.E.) and Postviral fatigue syndrome - presently classified in the Chapter on Diseases of the nervous system [at G93.3] – to be retained in that chapter of the forthcoming ICD-11.
Along with commending the proposal’s intention to highlight and reinforce the severe and devastating impact of M.E., we would like to draw attention to the body of scientific material referred to in the rationale for the proposal [Rationale point 1: Scientific evidence that exists for neurological dysfunction; Rationale point 2: Recent federal agency reviews and scientific evidence].
This reflects growing evidence of neurological, immunological and endocrinological dysfunction and related biomarkers. However, we agree that current scientific evidence of neurological impairment and WHO/ICD Revision's position on precedence [i.e. “legacy should trump with regard to the question of moving certain conditions to new chapters”] supports retention of chronic fatigue syndrome and myalgic encephalomyelitis in Diseases of the nervous system.
We support the proposal to move Postviral fatigue syndrome to a synonym under the Concept Title ‘Myalgic encephalomyelitis’. This recognises that not all instances of M.E. may result from a viral infection. We also agree with the proposed removal of the word ‘benign’ from the M.E. title, in keeping with the considerable medical complexity of this condition and its severe and lasting impact on patients.
The position in respect of ‘Chronic fatigue syndrome’ (CFS) is more complex:
· CFS is listed in the WHO ICD-10 index only.
· It is indexed to G93.3. Yet in practice the label ‘CFS’ is applied variably - both in research (with a multiplicity of definitions in use) and clinically.
Given the placement of ‘Fatigue syndrome’ in the WHO ICD-10 Mental and behavioural chapter [as a synonym under ‘Neurasthenia’ at F48.0], it was all but inevitable that the introduction of the term ‘Chronic fatigue syndrome’ to apply to a physical illness would cause confusion.
The confusion has a considerable impact on patients. For example, we are aware that some patients are being referred to services for ‘medically unexplained symptoms’, under the mistaken assumption that M.E. is a ‘functional somatic syndrome’. Indeed, the Joint Commissioning Panel for Mental Health (England) has recently published guidance stating that ‘Chronic Fatigue Syndrome/Myalgic Encephalomyelitis’ is a ‘functional somatic syndrome’ [Guidance for commissioners of services for people with medically unexplained symptoms 2017].
As the evidence gathered by this proposal so clearly demonstrates, this illness is a "serious, chronic, complex, and multisystem disease" that causes significant impairment - including neurological, cognitive, immunological, autonomic and energy metabolism disorder. We consider that it is vital that the WHO ICD continues to provide a bulwark against medical mismanagement of M.E. patients.
In this regard securing appropriate exclusions is vital, and we endorse the proposal’s recommendations, as set out at Note 4. In particular, we note that the ICD revision intends that the F48.0 Neurasthenia category [where ‘Fatigue syndrome’ presently appears], together with almost all of the present F45 somatoform disorder categories, be subsumed in a single new category - currently suggested name ‘Bodily distress disorder'. We agree that there needs to be reciprocal exclusions for M.E. and for CFS for the ‘Bodily distress disorder’ category.
We also agree that reciprocal exclusions for M.E. and for CFS for the category ‘Fatigue’ [previously ‘Malaise and fatigue’] are essential.
Forward ME 2017-Apr-21 - 14:01 UTC
--------------------
A PDF of Forward-ME's response (with key links on the second page) can be downloaded here:
https://dxrevisionwatch.files.wordpress.com/2017/04/forward-me1.pdf