Suzy Chapman and Mary Dimmock submitted a Proposal for classification of the G93.3 legacy categories for ICD-11
There's a deadline, today.
In order to be considered for inclusion in the final version of ICD-11, proposals need to be submitted by today, Thursday, March 30.
Over the past few weeks, Mary Dimmock and I have collaborated on the preparation of a formal proposal and rationale for the restructure of the ICD-10 G93.3 category terms:
Postviral fatigue syndrome;
Benign myalgic encephalomyelitis; and
Chronic fatigue syndrome.
On Sunday, March 26, after a
four year absence from the draft, "Team WHO" unexpectedly restored the G93.3 terms to the Beta platform.
They also approved my long standing proposal for exclusions under Fatigue for
Benign myalgic encephalomyelitis and
Chronic fatigue syndrome (though not yet for
Postviral fatigue syndrome).
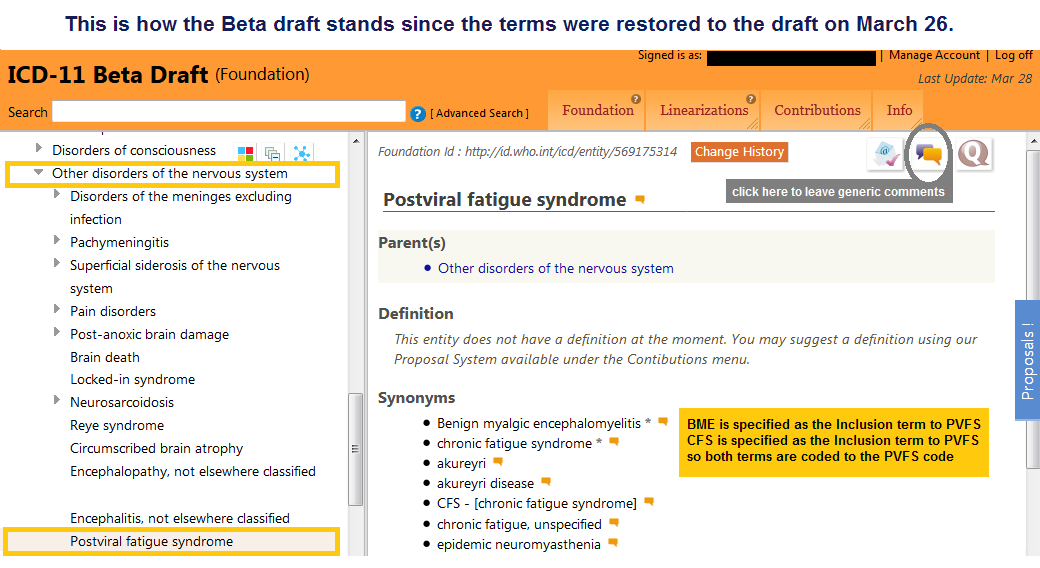
The terms were returned to their 2009 Beta location* with the caveat:
"While the optimal place in the classification is still being identified, the entity has been put back to its original place in ICD."
All three terms are currently back under the Neurology chapter, under parent:
Other disorders of the nervous system, with PVFS as the lead (or concept title) term, and BME and CFS specified as inclusions. The other content on the listing is much as it had stood in 2009.
Click here to view their listing on the Beta draft
I'm viewing this restoration as a "placeholder" while the work group continues to work towards consensus and we might expect revised proposals at some point in the future.
*In the ICD-11 Beta, as it had stood in early 2013, when they removed the terms from view in the public version of the drafting platform, they had been proposing CFS as the lead (concept title) term, with BME as the inclusion term, and PVFS under synonyms to CFS.
We submitted our Proposal on Monday - in good time for today's deadline.
In order to view our Proposal in the Beta "Proposal Mechanism" you will first need to register with the Beta platform.
You can register for access here:
http://bit.ly/2n7Kdj4
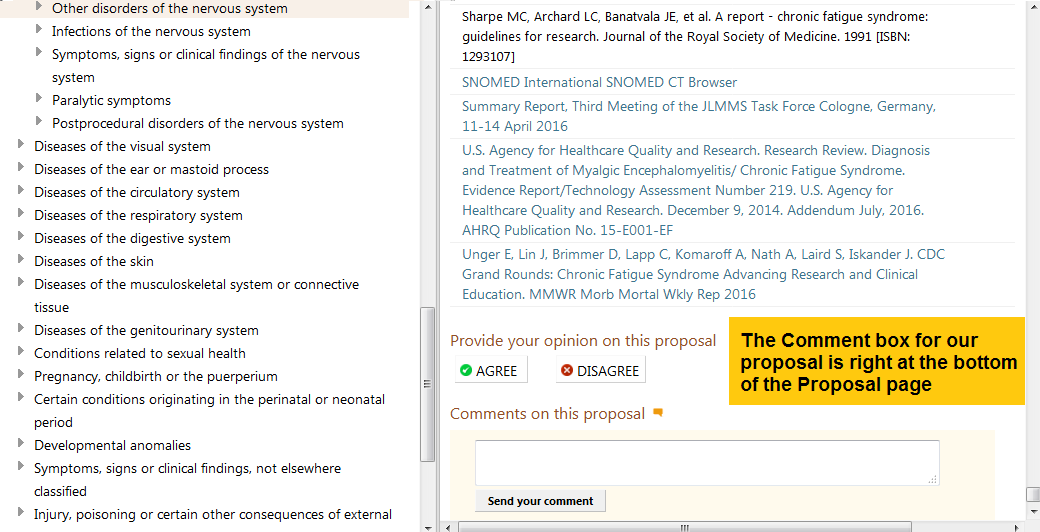
Once you are registered and logged in, this is the URL for viewing and commenting on our Proposal:
http://bit.ly/2n8I9qc
But for ease of access, we've put a copy of our Proposal and Rationale into a PDF, which you can download from my website here:
http://bit.ly/2mQxWTS
I have also attached a copy to this post.
When submitting for a complex restructure of the hierarchy or relationship between a group of ICD terms, rationales for proposals need to be provided - so it's not a quick read.
I'm posting just the first four pages for you which set out the proposed restructure. For the Notes and Rationales that support our recommendations, see the full
Proposal Document.
In the next post I will post instructions for commenting on proposals.
______________________________________________________________________________
Page 1
Proposal for the ICD-10 G93.3 legacy terms for ICD-11
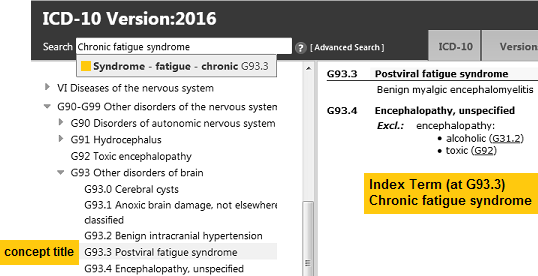
How the G93.3 terms are currently represented in ICD-10: (CFS is included in the Index, only.)
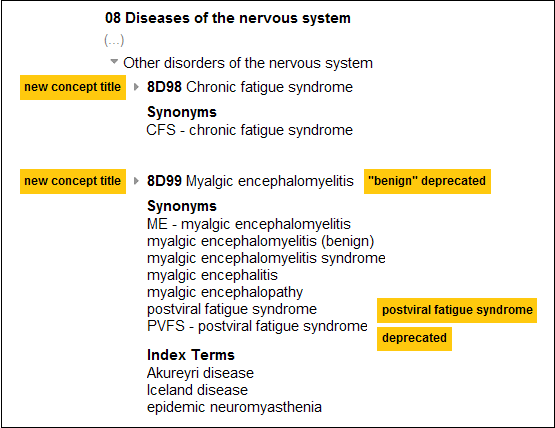
Our Proposal for ICD-11: (CFS and ME assigned to separate codes; PVFS under Synonyms to ME. "Benign" dropped.)
Codes for illustrative purposes only; Beta draft codes change daily as terms are added or reorganized.
_____________________________________________________________________________
Page 2
Complex Hierarchical Changes Proposal
Other disorders of the nervous system
Proposal submitted to ICD-11 Revision on March 27, 2017
Detailed Explanation of the Proposal
This Complex Hierarchical Changes Proposal is for the ICD-10 legacy entities coded and indexed to G93.3.
Declarations: This submission has been prepared by Mary Dimmock and Suzy Chapman. Mary Dimmock serves on the Board of Solve ME/CFS Initiative and also works with other ME organizations. Suzy Chapman has no affiliations. This proposal has been submitted in personal capacities and not on behalf of any organizations. The authors declare no conflicts of interest.
In ICD-10 Volume 1: Tabular List, the G93.3 ICD concept title is
Postviral fatigue syndrome; the inclusion term is
Benign myalgic encephalomyelitis.
Chronic fatigue syndrome is included in Volume 3: Alphabetical Index, only, and is indexed to G93.3.
In the absence of any proposals or rationales published by Topic Advisory Group (TAG) for Neurology, or by any other TAG, or by the ICD-11 MMS Joint Task Force during the preparation of this submission, the authors propose the restructuring of these entities taking their classification within ICD-10 Version: 2016 as the reference point [1].
Recommendation: For ICD-11, the G93.3 legacy entities should be retained under
Chapter 08: Diseases of the nervous system. (See Rationale 3.2)
In ICD-10 Volume 1: Tabular List, the concept title is a child entity under parent class:
Other disorders of brain.
In May 2010, a change of hierarchy for the ICD-10 G93.3 legacy entities was recorded in the iCAT (Collaborative Authoring Tool). Parent:
Other disorders of brain was removed and replaced with parent:
Other disorders of the nervous system [2].
Recommendation: For ICD-11, the G93.3 legacy entities should be retained under parent:
Other disorders of the nervous system. (See Rationale 3.3)
The following changes to the hierarchy between the three entities are proposed:
Add new Concept Title: Chronic fatigue syndrome (See Note 1)
Remove Concept Title: Postviral fatigue syndrome
Add new Concept Title: Benign myalgic encephalomyelitis (See Rationale 3.4)
Replace new Concept Title: Benign myalgic encephalomyelitis with Myalgic encephalomyelitis (See Note 2)
Add: Postviral fatigue syndrome under Synonyms to new Concept Title: Myalgic encephalomyelitis (See Note 3)
Assign unique sequential codes to each new Concept Title.
These new Concept Titles are proposed to be listed in the
Foundation,
MMS Linearization, and
Special tabulation neurological conditions linearization.
References:
1 International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) Version: 2016.
http://apps.who.int/classifications/icd10/browse/2016/en#/G93.3 [Accessed March 12, 2017]
2 Change history, iCAT (Collaborative Authoring Tool) drafting platform, May 1, 2010. [Accessed May 24, 2010]
_____________________________________________________________________________
Pages 3 and 4
Proposed hierarchical restructure:
1. ICD Concept Title
1.1 Fully Specified Name: Chronic fatigue syndrome
2. Classification Properties
2.1 Parents: Primary: Diseases of the nervous system > Other disorders of the nervous system
2.2 Type
Disease
Disorder / Syndrome
2.3 Use and Linearizations
Use: Primary Care / Clinical / Research
Linearization(s): Morbidity / Mortality / Neurology
3. Textual Definition(s)
[See Rationale 2 and 4]
4.1.1 Synonyms (See Note 3.1)
CFS - [chronic fatigue syndrome]
4.2 Inclusions
There are no inclusions for this entity
4.3 Exclusions (See Note 4)
--------------------------------------------------------------
1. ICD Concept Title
1.1 Fully Specified Name: Myalgic encephalomyelitis
2. Classification Properties
2.1 Parents: Primary: Diseases of the nervous system > Other disorders of the nervous system
2.2 Type
Disease
Disorder / Syndrome
2.3 Use and Linearizations
Use: Primary Care / Clinical / Research
Linearization(s): Morbidity / Mortality / Neurology
3. Textual Definition(s)
[See Rationale 2 and 4]
4.1.1 Synonyms (See Note 3.1)
ME - [myalgic encephalomyelitis]
myalgic encephalomyelitis (benign)
myalgic encephalomyelitis syndrome
myalgic encephalitis
myalgic encephalopathy
postviral fatigue syndrome
PVFS - [postviral fatigue syndrome]
4.2 Inclusions
There are no inclusions for this entity
4.3 Exclusions (See Note 4)
The authors recommend the following historical terms for inclusion in the Index:
Index terms
Akureyri disease
Iceland disease
epidemic neuromyasthenia
Notes:
Note 1: Inclusion of chronic fatigue syndrome in Foundation and MMS Linearization: The authors support the principle set out in ICD-10 Volume 2: Instruction Manual (2010):
"The categories have to be chosen to facilitate the statistical study of disease phenomena. A specific disease entity that is of particular public health importance, or that occurs frequently, should have its own category." [1]. The authors support the precedent set by the Canadian Institute for Health Information (CIHI) that is responsible for the development, update and maintenance of ICD-10-CA, and the German Institute of Medical Documentation and Information (DIMDI) that is responsible for the development, update and maintenance of ICD-10-GM in adding chronic fatigue syndrome to their Tabular Lists.
References:
1 International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Volume 2 Instruction Manual, 2010 Edition.
http://www.who.int/classifications/icd/ICD10Volume2_en_2010.pdf
2 International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada, Volume One ‒ Tabular List, Canadian Institute for Health Information 2015.
http://assets.ibc.ca/Documents/Auto Insurance/ICD-10-CA 2015.pdf
3 Internationale statistische Klassifikation der Krankheiten und verwandter Gesundheitsprobleme 10. Revision German Modification Version 2017.
https://www.dimdi.de/static/de/klassi/icd-10-gm/kodesuche/onlinefassungen/htmlgm2017
etc.
For full Notes and Rationale: http://bit.ly/2mQxWTS
_____________________________________________________________________________
A caveat about our recommendations: Our proposal recommends that ME and CFS are not listed under
Postviral fatigue syndrome and are assigned unique codes. We have also requested reciprocating exclusions for
Fatigue, and for
Bodily distress disorder; and that the designation, "Benign" is deprecated.
We appreciate that many, including the IOM, have expressed concerns with the term "CFS." But realistically, it cannot be removed at this time because it is still used clinically and for social security and insurance purposes. Additionally, WHO requires statistical continuity from one ICD edition to another. During the transition period, which will span several years since member states will set their own timescales for implementation, WHO will be collecting data from both ICD-10 and ICD-11.
Once ICD-11 is released, it will be placed on an annual update and revision schedule (the first in 2019). Our understanding is that WHO intends that the platform will remain open for suggestions for revisions from stakeholders, as well as from member states and collaborating centres. Ongoing and future scientific developments will inform the annual revisions to the classification.
In the next post: How to comment on our proposal, and on the Beta as it currently stands.
I shall be busy over the next few days and won't be monitoring my Phoenix Rising Inbox. If you have queries in relation to the Beta, please shoot me an email via my website
Contact Form and I'll get back to you as soon as I can.


 THANK YOU so very much for all of your hard work, words cannot express my gratitude. You are, indeed, a hero.
THANK YOU so very much for all of your hard work, words cannot express my gratitude. You are, indeed, a hero.