Dx Revision Watch
Suzy Chapman Owner of Dx Revision Watch
- Messages
- 3,061
- Location
- UK
***********************************************************************************************
Edited to add two summary posts on Dx Revision Watch site:
Two ICD-11 G93.3 updates on Dx Revision Watch:
A proposal for the ICD-10 G93.3 legacy terms for ICD-11: Part Two http://wp.me/pKrrB-4eH
http://wp.me/pKrrB-4eH
and for background to the proposal:
A proposal for the ICD-10 G93.3 legacy terms for ICD-11: Part One http://wp.me/pKrrB-4dV
http://wp.me/pKrrB-4dV
http://wp.me/pKrrB-4dV
*************************************************************************************************
Update on status of ICD-11 for the G93.3 ICD-10 legacy terms
The revision of ICD-10 and development of the structure for ICD-11 and its associated publications launched in 2007.
The original dissemination date for ICD-11 had been projected for 2012. This was rapidly revised to 2015, then postponed to 2017 and is currently 2018. The scope of the project has been scaled back but there is still a great deal of work to be completed.
The revision was being overseen by a Revision Steering Group. In 2015, the ICD-11 MMS Joint Task Force was assembled to oversee the finalization of ICD-11.
The project remains underfunded and under resourced and the Joint Task Force is struggling with the workload required to release a stable version of ICD-11 in 2018.
There is the possibility of a further postponement. But until any announcement is made by WHO, it should be assumed that the date of 2018 stands.
The WHO is intending to present an incomplete version of ICD-11 to the WHA in May 2018. The WHO won't be seeking endorsement from WHA until later, but plans to release a version of ICD-11 at some point after May 2018.
No firm date has been issued and it is unclear how many of the associated publications, for example, the print editions for the specialty versions (which will include Neurology) or the abridged Primary Care version of the Mental or behavioural disorders chapter (ICD-11 PHC), will be ready by then.
No mandatory implementation date
Once released, Member States will need to evaluate ICD-11 and begin to plan for transition from ICD-10. This will take most countries several years. It is likely to take longer for those countries who use a modification of the ICD, for example the USA and Canada, to develop modifications of the new edition. There is no mandatory implementation date and Member States will transition at their own pace and in the meantime, ICD-10 will continue to be used for data reporting.
Proposals deadline
Dozens of proposals for new and existing terms are being uploaded to the Beta draft daily, which will all need processing.
According to the newsletter: ICD-11 Update, January 2017:
"Proposals that are received between 1 January 2017 and 30 March 2017 will be taken into account for the final version for implementation. Proposals received after that date will be considered in the context of ICD-11 maintenance after 2018."
(Comments by Member States and improvements arising as a part of the Quality Assurance mechanism will be included with deadlines later in 2017.)
"It will be all over by Christmas..."
In June, 2015, I had a teleconference with Dr Robert Jakob, facilitated by Project Manager, Anneke Schmider. During our discussions, Dr Jakob advised me that he anticipated Topic Advisory Group (TAG) Neurology would release their proposals for the classification of the G93.3 legacy terms in September 2015, and if not ready by September, then by "December 2015, at the latest" - thereby allowing time for stakeholder scrutiny and comment prior to finalization.
In July 2015, Mary Dimmock and I provided Dr Jakob, with his agreement, a number of reports, research study references, conference presentations and other materials to be passed to TAG Neurology to inform the process.
However, no proposals and rationales for proposals have been published by TAG Neurology via the Proposal Mechanism, or entered into the Beta draft or released by any other means, and the terms remain unaccounted for in any chapter and any linearization of the public draft.
How the draft had stood in early 2013
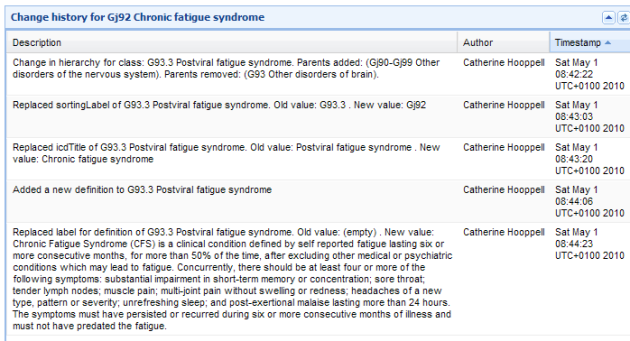
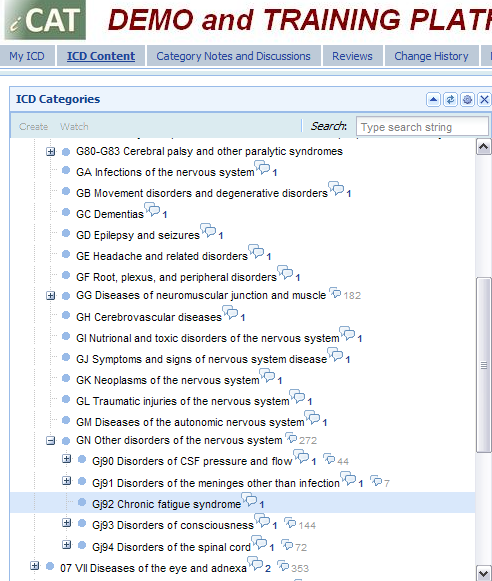
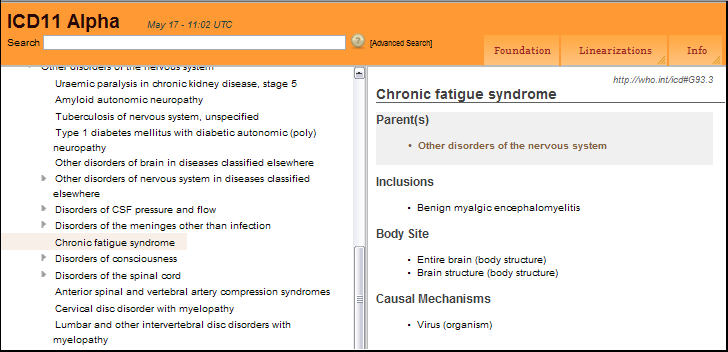
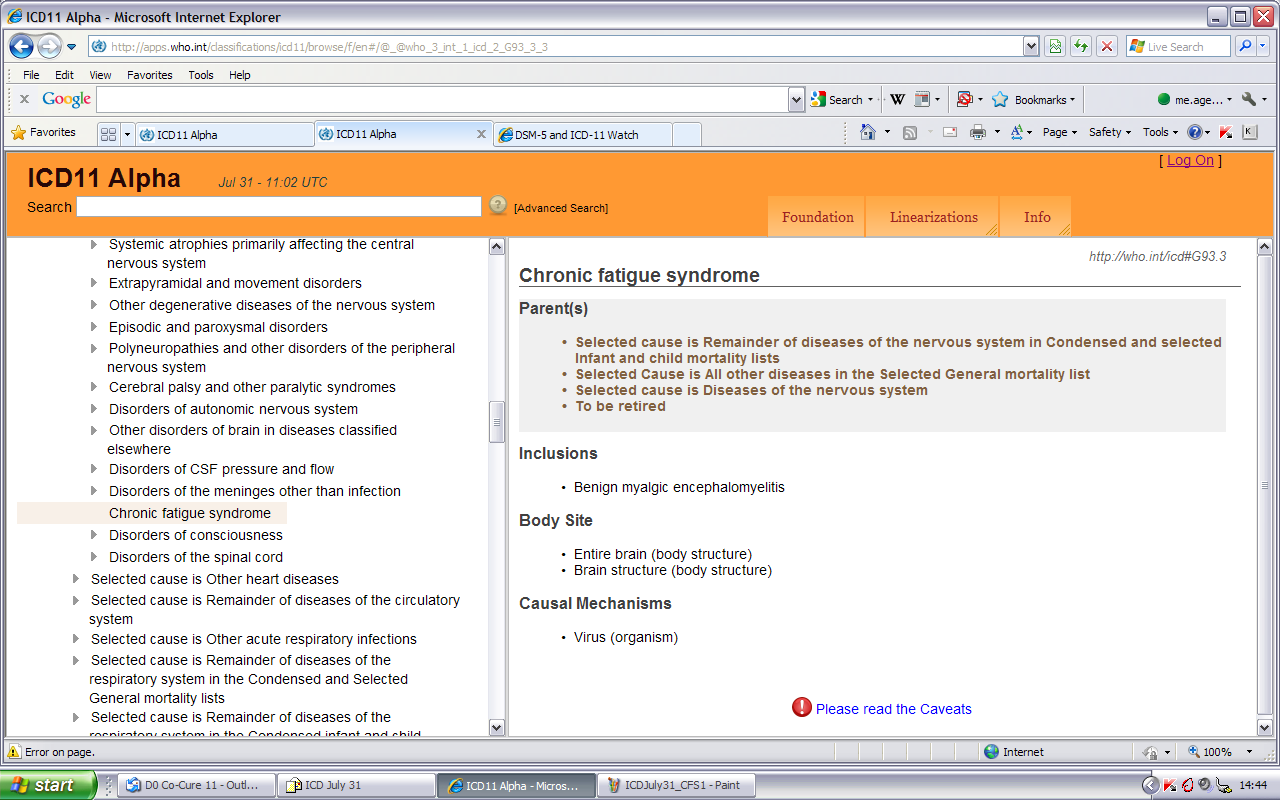
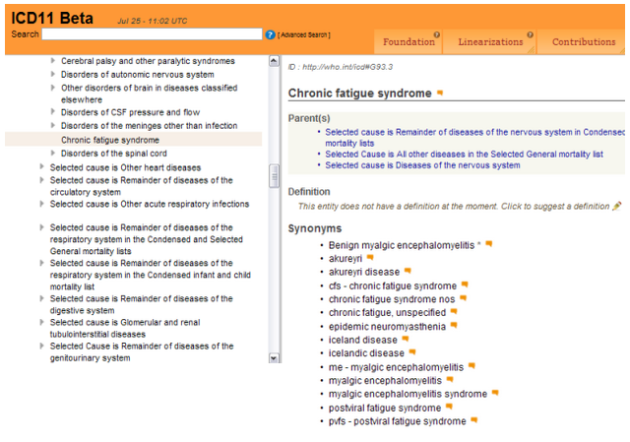
In early 2013, when the three terms were last seen in the Beta draft, the proposal had been for CFS to become the new lead code term, with BME specified as the inclusion term, and with PVFS under Synonyms.
(I have screenshots tracking the revision of these terms in the iCAT, Alpha and Beta phases up to early 2013, which I shall add to the thread later.)
However, it was unclear at the time under what parent term these were proposed to sit or whether it was proposed to locate the terms under a different chapter. All three terms were subsequently taken out of the public version of the draft and there have been no progress reports since.
Request that Joint Task Force expedite release of proposals
I was aware that the Joint Task Force (JTF) had a three day meeting scheduled for 20-22 February, in Cologne.
I wrote to the JTF on February 6 and requested that the absence of TAG proposals for these three terms was tabled for discussion at a Joint Task Force meeting with the objective of expediting the release of TAG Neurology's proposals prior to March 2017.
This would give stakeholders the opportunity to review and comment on proposals while there is still time, and in order that ICD-11 is inclusive of stakeholder participation in the revision process.
A number of international patient organizations were approached and asked if they would also contact those JTF members in their own countries in support of my call for the urgent release of TAG Neurology's proposals.
16 international organizations have confirmed that they have done so and I would like to publicly thank them for their support with this.
Continued lack of transparency
To date, I have received no response from the JTF co-chairs to my initial letter of February 6, or two follow up letters on February 22 and 23.
Some organizations did receive responses from members of the JTF, but none from the co-chairs.
It was confirmed in one of these responses that I had been successful in getting the matter discussed at the Wednesday, February 22 meeting, but no information was given about the outcome of that discussion.
Some vague information was given in one response but it is unconfirmed, may be incomplete and may not be up to date; I cannot rely on this information until the co-chairs of the Joint Task Force have fully clarified the current proposals for these terms.
Parliamentary Written Question
At the weekend, I approached the Countess of Mar with a briefing on the situation and a suggestion that possibly a Parliamentary Written Question might force the information we require into the public domain.
Lady Mar confirmed last night that she had tabled a Written Question on Monday and it was published overnight. I will post a copy in the next post.
I have some further posts to add to this thread but I need to edit a document today so I will add these to the thread on Wednesday.
Suzy Chapman
Edited to add two summary posts on Dx Revision Watch site:
Two ICD-11 G93.3 updates on Dx Revision Watch:
A proposal for the ICD-10 G93.3 legacy terms for ICD-11: Part Two http://wp.me/pKrrB-4eH
http://wp.me/pKrrB-4eH
and for background to the proposal:
A proposal for the ICD-10 G93.3 legacy terms for ICD-11: Part One http://wp.me/pKrrB-4dV
http://wp.me/pKrrB-4dV
http://wp.me/pKrrB-4dV
*************************************************************************************************
Update on status of ICD-11 for the G93.3 ICD-10 legacy terms
The revision of ICD-10 and development of the structure for ICD-11 and its associated publications launched in 2007.
The original dissemination date for ICD-11 had been projected for 2012. This was rapidly revised to 2015, then postponed to 2017 and is currently 2018. The scope of the project has been scaled back but there is still a great deal of work to be completed.
The revision was being overseen by a Revision Steering Group. In 2015, the ICD-11 MMS Joint Task Force was assembled to oversee the finalization of ICD-11.
The project remains underfunded and under resourced and the Joint Task Force is struggling with the workload required to release a stable version of ICD-11 in 2018.
There is the possibility of a further postponement. But until any announcement is made by WHO, it should be assumed that the date of 2018 stands.
The WHO is intending to present an incomplete version of ICD-11 to the WHA in May 2018. The WHO won't be seeking endorsement from WHA until later, but plans to release a version of ICD-11 at some point after May 2018.
No firm date has been issued and it is unclear how many of the associated publications, for example, the print editions for the specialty versions (which will include Neurology) or the abridged Primary Care version of the Mental or behavioural disorders chapter (ICD-11 PHC), will be ready by then.
No mandatory implementation date
Once released, Member States will need to evaluate ICD-11 and begin to plan for transition from ICD-10. This will take most countries several years. It is likely to take longer for those countries who use a modification of the ICD, for example the USA and Canada, to develop modifications of the new edition. There is no mandatory implementation date and Member States will transition at their own pace and in the meantime, ICD-10 will continue to be used for data reporting.
Proposals deadline
- There is a deadline of March 30 for consideration of proposals from the various working groups that were assembled in 2008 to work on revising ICD chapters for ICD-11.
Dozens of proposals for new and existing terms are being uploaded to the Beta draft daily, which will all need processing.
According to the newsletter: ICD-11 Update, January 2017:
"Proposals that are received between 1 January 2017 and 30 March 2017 will be taken into account for the final version for implementation. Proposals received after that date will be considered in the context of ICD-11 maintenance after 2018."
(Comments by Member States and improvements arising as a part of the Quality Assurance mechanism will be included with deadlines later in 2017.)
"It will be all over by Christmas..."
In June, 2015, I had a teleconference with Dr Robert Jakob, facilitated by Project Manager, Anneke Schmider. During our discussions, Dr Jakob advised me that he anticipated Topic Advisory Group (TAG) Neurology would release their proposals for the classification of the G93.3 legacy terms in September 2015, and if not ready by September, then by "December 2015, at the latest" - thereby allowing time for stakeholder scrutiny and comment prior to finalization.
In July 2015, Mary Dimmock and I provided Dr Jakob, with his agreement, a number of reports, research study references, conference presentations and other materials to be passed to TAG Neurology to inform the process.
However, no proposals and rationales for proposals have been published by TAG Neurology via the Proposal Mechanism, or entered into the Beta draft or released by any other means, and the terms remain unaccounted for in any chapter and any linearization of the public draft.
How the draft had stood in early 2013
In early 2013, when the three terms were last seen in the Beta draft, the proposal had been for CFS to become the new lead code term, with BME specified as the inclusion term, and with PVFS under Synonyms.
(I have screenshots tracking the revision of these terms in the iCAT, Alpha and Beta phases up to early 2013, which I shall add to the thread later.)
However, it was unclear at the time under what parent term these were proposed to sit or whether it was proposed to locate the terms under a different chapter. All three terms were subsequently taken out of the public version of the draft and there have been no progress reports since.
- The G93.3 legacy terms have now been missing from the public version of the Beta draft for four years.
- Until TAG Neurology releases its proposals for these legacy terms, stakeholders are unable to review, comment on or input into TAG proposals for chapter location(s), parent class(es), hierarchies, or Content Model parameters.
- Nor is is possible for stakeholders to submit proposals for Exclusions for these terms under other diagnostic categories, since these entities do not currently appear in the draft.
Request that Joint Task Force expedite release of proposals
I was aware that the Joint Task Force (JTF) had a three day meeting scheduled for 20-22 February, in Cologne.
I wrote to the JTF on February 6 and requested that the absence of TAG proposals for these three terms was tabled for discussion at a Joint Task Force meeting with the objective of expediting the release of TAG Neurology's proposals prior to March 2017.
This would give stakeholders the opportunity to review and comment on proposals while there is still time, and in order that ICD-11 is inclusive of stakeholder participation in the revision process.
A number of international patient organizations were approached and asked if they would also contact those JTF members in their own countries in support of my call for the urgent release of TAG Neurology's proposals.
16 international organizations have confirmed that they have done so and I would like to publicly thank them for their support with this.
Continued lack of transparency
To date, I have received no response from the JTF co-chairs to my initial letter of February 6, or two follow up letters on February 22 and 23.
Some organizations did receive responses from members of the JTF, but none from the co-chairs.
It was confirmed in one of these responses that I had been successful in getting the matter discussed at the Wednesday, February 22 meeting, but no information was given about the outcome of that discussion.
Some vague information was given in one response but it is unconfirmed, may be incomplete and may not be up to date; I cannot rely on this information until the co-chairs of the Joint Task Force have fully clarified the current proposals for these terms.
Parliamentary Written Question
At the weekend, I approached the Countess of Mar with a briefing on the situation and a suggestion that possibly a Parliamentary Written Question might force the information we require into the public domain.
Lady Mar confirmed last night that she had tabled a Written Question on Monday and it was published overnight. I will post a copy in the next post.
I have some further posts to add to this thread but I need to edit a document today so I will add these to the thread on Wednesday.
Suzy Chapman
Last edited: