

Legendrew submitted a new blog post:
Hyperparathyroidism: An Often Overlooked Differential Diagnosis to ME/CFS
Andrew Gladman puts hyperparathyroidism under the microscope, exploring what the disease is, how it can mimic ME/CFS in presentation and how it is treated.
Chronic fatigue syndrome or ME/CFS is, whether we like it or not, by current definition a diagnosis of exclusion. The biggest diagnostic task is therefore differentiating it from the plethora of other disorders that also have a fatigue component.
ME/CFS may be distinguished from other causes of fatigue on the basis of certain presenting symptoms such as cognitive dysfunction, which is not present in almost all other fatigue-producing disorders. Once a specific cause of fatigue has been diagnosed, CFS is then excluded, by definition.
The problem that arises, however, is that almost any chronic illness that produces extensive disability and fatigue may be included in the differential diagnosis. Therefore it is very difficult to ensure that everything is adequately ruled out before a diagnosis of ME/CFS is reached.
This diagnosis of exclusion is often a very time-consuming and expensive task. For these reasons the diagnosis of ME/CFS is often given somewhat prematurely.
Conditions that can cause fatigue include the following:
Often mistaken for its close namesake, hyperthyroidism, hyperparathyroidism in fact has nothing in common with the thyroid in function, and is so named because the troublesome gland in question simply lies in such close proximity to the thyroid.
There are two different types of hyperparathyroidism: primary and secondary.
Primary hyperparathyroidism is caused by one or more benign tumours (adenomas) of the parathyroid glands. Normally these glands control blood calcium levels by secreting parathyroid hormone (PTH) when blood calcium levels drop beyond the normal range.
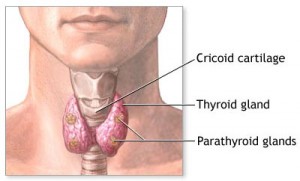
Diagram showing location of parathyroid glands
The symptoms of hyperparathyroidism include weakness and fatigue, depression, bone pain/osteoporosis, muscle soreness (myalgias), nausea/vomiting, constipation, headaches, frequent urination (polyuria) and kidney stones.
The symptoms typically develop slowly. However, they may appear very suddenly and severely. This is often known as a parathyroid crisis and can be fatal if left untreated.
Hyperparathyroidism is also associated with a high risk of pancreatitis (both acute and chronic) which can cause acute abdominal symptoms such as cramping, nausea and diarrhea.
Furthermore, hyperparathyroidism is very often seen in combination with a vitamin D deficiency which can make diagnosis somewhat more difficult. From the above list alone, it is clear to see why hyperparathyroidism should always be tested for in ME/CFS patients, given the similarity of the symptom presentation.
The tests for this condition are blood calcium which shows as unusually high, parathyroid hormone levels which are very high, alkaline phosphatase which can sometimes be elevated, vitamin D levels which are very often low and phosphate which is also sometimes low.
Testing can prove difficult however, with calcium and PTH levels fluctuating quite wildy. This however is quite indicative of the condition, as under normal circumstances calcium and PTH remain very consistent. If hyperparathyroidism is suspected, then a scan will be recommended to try and see whether there is a visible tumour present, although diagnosis is made through blood tests alone.
As previously mentioned, there is also a condition known as secondary hyperparathyroidism, in which PTH levels are elevated. However, this only usually occurs in patients with chronic renal failure, abnormally low levels of calcium (hypocalcemia) and sometimes as a result of vitamin D deficiency. This is normally differentiated from primary hyperparathyroidism by correcting the deficiency and observing the calcium and PTH level response.
The first line of treatment for primary hyperparathyroidism for the majority of patients is a minor surgery, under general anesthesia, to remove the tumour which in turn removes the PTH excess and allows the calcium levels to return to normal.
This is not a major surgery, with the majority being done today via keyhole surgery, and is usually undertaken as an outpatient procedure. This surgery also boasts impressive cure rates as high as 95% with the remaining 5% often having another parathyroid tumour which was missed during the first surgery.
Of all the missed diagnoses of ME/CFS and fibromyalgia, primary hyperparathyroidism proves to be one of the most tragic simply as a result of how treatable the condition is relative to the suffering it can cause.
If any of the symptoms sound somewhat familiar, be sure to mention this to your primary care physician. A couple of simple blood tests could lead you to a long overdue answer to your personal health problems!
For more information on hyperparathyroidism be sure to visit Parathyroid.com.
Phoenix Rising is a registered 501 c.(3) non profit. We support ME/CFS and NEID patients through rigorous reporting, reliable information, effective advocacy and the provision of online services which empower patients and help them to cope with their isolation.
There are many ways you can help Phoenix Rising to continue its work. If you feel able to offer your time and talent, we could really use some more authors, proof-readers, fundraisers, technicians etc. and we'd love to expand our Board of Directors. So, if you think you can help then please contact Mark through the Forum.
And don't forget: you can always support our efforts at no cost to yourself as you shop online! To find out more, visit Phoenix Rising’s Donate page by clicking the button below.
 Continue reading the Original Blog Post
Continue reading the Original Blog Post
Hyperparathyroidism: An Often Overlooked Differential Diagnosis to ME/CFS
Andrew Gladman puts hyperparathyroidism under the microscope, exploring what the disease is, how it can mimic ME/CFS in presentation and how it is treated.
Chronic fatigue syndrome or ME/CFS is, whether we like it or not, by current definition a diagnosis of exclusion. The biggest diagnostic task is therefore differentiating it from the plethora of other disorders that also have a fatigue component.
ME/CFS may be distinguished from other causes of fatigue on the basis of certain presenting symptoms such as cognitive dysfunction, which is not present in almost all other fatigue-producing disorders. Once a specific cause of fatigue has been diagnosed, CFS is then excluded, by definition.
The problem that arises, however, is that almost any chronic illness that produces extensive disability and fatigue may be included in the differential diagnosis. Therefore it is very difficult to ensure that everything is adequately ruled out before a diagnosis of ME/CFS is reached.
This diagnosis of exclusion is often a very time-consuming and expensive task. For these reasons the diagnosis of ME/CFS is often given somewhat prematurely.
Conditions that can cause fatigue include the following:
- Chronic heart disease
- Psychiatric illnesses
- Thyroid diseases
- Connective tissue diseases
- Chronic anemia
- Neoplastic (cancerous) disease
- Chronic infections (e.g., HIV/AIDS)
- Endocrine diseases (e.g., Addison disease)
- Inflammatory bowel disease
- Drug abuse
- Liver disease
- Renal disease
Often mistaken for its close namesake, hyperthyroidism, hyperparathyroidism in fact has nothing in common with the thyroid in function, and is so named because the troublesome gland in question simply lies in such close proximity to the thyroid.
There are two different types of hyperparathyroidism: primary and secondary.
Primary hyperparathyroidism is caused by one or more benign tumours (adenomas) of the parathyroid glands. Normally these glands control blood calcium levels by secreting parathyroid hormone (PTH) when blood calcium levels drop beyond the normal range.

Diagram showing location of parathyroid glands
PTH stimulates the release of calcium from the bones and also stimulates the conversion of inactive vitamin D to active vitamin D, which aids in the digestion of calcium. When an adenoma is present, very high levels of PTH are released which results in a high level of blood calcium. It is this hypercalcemia which is thought to produce the symptoms.The symptoms of hyperparathyroidism include weakness and fatigue, depression, bone pain/osteoporosis, muscle soreness (myalgias), nausea/vomiting, constipation, headaches, frequent urination (polyuria) and kidney stones.
The symptoms typically develop slowly. However, they may appear very suddenly and severely. This is often known as a parathyroid crisis and can be fatal if left untreated.
Hyperparathyroidism is also associated with a high risk of pancreatitis (both acute and chronic) which can cause acute abdominal symptoms such as cramping, nausea and diarrhea.
Furthermore, hyperparathyroidism is very often seen in combination with a vitamin D deficiency which can make diagnosis somewhat more difficult. From the above list alone, it is clear to see why hyperparathyroidism should always be tested for in ME/CFS patients, given the similarity of the symptom presentation.
The tests for this condition are blood calcium which shows as unusually high, parathyroid hormone levels which are very high, alkaline phosphatase which can sometimes be elevated, vitamin D levels which are very often low and phosphate which is also sometimes low.
Testing can prove difficult however, with calcium and PTH levels fluctuating quite wildy. This however is quite indicative of the condition, as under normal circumstances calcium and PTH remain very consistent. If hyperparathyroidism is suspected, then a scan will be recommended to try and see whether there is a visible tumour present, although diagnosis is made through blood tests alone.
As previously mentioned, there is also a condition known as secondary hyperparathyroidism, in which PTH levels are elevated. However, this only usually occurs in patients with chronic renal failure, abnormally low levels of calcium (hypocalcemia) and sometimes as a result of vitamin D deficiency. This is normally differentiated from primary hyperparathyroidism by correcting the deficiency and observing the calcium and PTH level response.
The first line of treatment for primary hyperparathyroidism for the majority of patients is a minor surgery, under general anesthesia, to remove the tumour which in turn removes the PTH excess and allows the calcium levels to return to normal.
This is not a major surgery, with the majority being done today via keyhole surgery, and is usually undertaken as an outpatient procedure. This surgery also boasts impressive cure rates as high as 95% with the remaining 5% often having another parathyroid tumour which was missed during the first surgery.
Of all the missed diagnoses of ME/CFS and fibromyalgia, primary hyperparathyroidism proves to be one of the most tragic simply as a result of how treatable the condition is relative to the suffering it can cause.
If any of the symptoms sound somewhat familiar, be sure to mention this to your primary care physician. A couple of simple blood tests could lead you to a long overdue answer to your personal health problems!
For more information on hyperparathyroidism be sure to visit Parathyroid.com.
Phoenix Rising is a registered 501 c.(3) non profit. We support ME/CFS and NEID patients through rigorous reporting, reliable information, effective advocacy and the provision of online services which empower patients and help them to cope with their isolation.
There are many ways you can help Phoenix Rising to continue its work. If you feel able to offer your time and talent, we could really use some more authors, proof-readers, fundraisers, technicians etc. and we'd love to expand our Board of Directors. So, if you think you can help then please contact Mark through the Forum.
And don't forget: you can always support our efforts at no cost to yourself as you shop online! To find out more, visit Phoenix Rising’s Donate page by clicking the button below.
Last edited by a moderator:

