

Simon submitted a new blog post:
Hunting down the cause of ME/CFS & other challenging disorders - Lipkin in London
Simon McGrath reports on Dr. Lipkin's talk to patients in London ...

Dr. W. Ian Lipkin
In a talk to patients in London on 3rd September, Dr. W. Ian Lipkin described the extraordinary lengths he and his team are prepared to go to in order to track down the source of an illness, with examples ranging from autism to the strange case of Kawasaki disease.
His talk emphasised the use of high-tech methods and following the evidence wherever it leads, before outlining his ME/CFS research programme that takes a similar approach. And he believes the action in his field is moving from acute illnesses such as SARS to chronic illnesses – including ME/CFS.
Lipkin is a renowned virus hunter who heads up the Center for Infection and Immunity at Columbia University. He’s discovered over 400 viruses, pioneered new molecular techniques for identifying pathogens, and helped the World Health Organisation and Chinese Ministry of Health deal with the SARS outbreak.
You may have seen one of Lipkin's many recent appearances in the media as an expert on Ebola. Yet he now says the future of his field lies not with acute infections, but in understanding the role microbes play in chronic diseases – one reason why ME/CFS has become a major focus his research.

Proving it
Once upon a time, proving a link between a pathogen and a disease was relatively straightforward. Usually it involved culturing a bug in the lab and showing the bug caused disease in animals too.
But for the most obviously infectious diseases like tuberculosis, smallpox or cholera, the responsible bugs have already been discovered. Lipkin and his team now hunt in more difficult territory, where linking disease with a microbial trigger is altogether more complicated.
Most microbes can’t be cultured in the lab, and often there isn’t an ‘animal model’ of the disease. How, asked Lipkin, would you create a mouse model for brain fog?
So the best way of demonstrating a microbe plays a key role in an illness such as ME/CFS is to show you can treat patients with drugs that target that microbe and that the patients improve or recover – or to find a vaccine that can prevent the illness. No doubt this is just the kind of proof that patients would most appreciate.
Intriguingly, Lipkin first encountered ME/CFS briefly in the 1980s while working as a physician in California, when Dr. Dan Peterson asked him to examine some of his Incline Village patients.
Fast forward to the 1990s and Lipkin had moved into research, and he was asked to investigate a suggested link between Borna disease virus (another virus he’d discovered) and ME/CFS.
He and Birgitta Evengard ran a large study, but found no link with the virus. However, the research did find evidence that ME/CFS patients had immune activation. “I was convinced that this was a biologically based problem, that it was not psychological”. Unfortunately there was no funding then to pursue further research into ME/CFS.
Still, he retained his interest, and when he was asked a few years ago to look at a link between the disease and another virus, this time XMRV/PMLV, he jumped at it. Again the link was disproved for that specific virus, but he’s continuing to hunt for viruses and other bugs as part of his latest programme of ME/CFS research.
Where new human viruses come from

Lipkin et al found 50 new viruses just in the Indian Flying Fox.
Lipkin has probably discovered more viruses than anyone, but he is well aware we’ve only found a fraction of the viral world.
Just how many unknown viruses are out there was highlighted by work Lipkin did as part of the U.S. Agency for International Development’s ‘Predict’ programme, an ambitious effort to find the next Ebola lurking in nature before it spreads out of control.
Most new human viruses start off life in wild mammals, and they often jump to humans via domesticated animals. New forms of flu, for example, often travel into humans from chickens that caught the virus from wild ducks. So one of Predict’s efforts was to estimate how many viruses there were in mammals – and they found a lot.
Taking a single bat species as an example, Lipkin and colleagues found 55 viruses — 50 of which had never been seen before. They detected the viruses from their DNA or RNA using high-throughput sequencing techniques that Lipkin helped pioneer.
Extrapolating from this work and more on other mammals, he and his collaborators conservatively estimated that there are 320,000 different viruses in mammals, most of them unknown.
That’s a pretty big pool of viruses that could produce the next human disease.
Linking Viruses to Human Disease
Some of these unknown viruses may play a role in ME/CFS — we don’t yet know. Showing that a particular virus causes a given disease requires detecting an immune response to the virus, particularly by finding the antibodies that help us fight off an infection.
Looking for antibodies has a huge advantage over looking for microbe DNA or RNA, because antibodies stick around long after the body has defeated the infection and the virus has vanished. Lipkin has previously called this approach of focusing on antibodies as looking for 'shadows of infection', something he’s keen to do in ME/CFS.
Just as there are microarray chips for detecting DNA or RNA of specific viruses, there are now ‘peptide microarrays’ that effectively allow researchers to check for antibodies against any virus. Peptides (i.e., short protein chains) can mimic every possible viral protein that antibodies might bind to.
“You can cover all vertebrate viruses in a single chip, which is amazing”, said Lipkin at the CMRC conference. When blood is run across the peptide-studded chip, the antibodies in the blood glom onto the peptides they’re associated with. And since each antibody was created in response to a particular virus, this reveals the (known) viruses that have ever infected the individual.
Lipkin used this method to great effect to study an outbreak of the MERS virus in the Middle East. He tested camel blood in Saudi Arabia with peptide microarray chips and found that the vast majority had at some point been infected with MERS. Added to other studies, this work showed that camels were the likely cause of the human MERS outbreak in the region.
Some outbreaks of disease are bug-free
In late 2007 a slaughterhouse processing 30 thousand pigs a day reported an outbreak of a neurological disease, and researchers began looking for the pathogen that caused it.
Lipkin and his colleagues realised that the patients worked at or near the section where workers blew brain tissue out of the pig skulls with a high pressure hose, a new technique that had been introduced when plant owners realized there was a market for brain matter in the Far East.
The result was a huge mess, including aerosolized bits of myelin, the fatty insulating sheath around nerve fibres. The workers’ immune systems, it turns out, were reacting hugely to this, triggering the paralysis or weak limbs and other neurological symptoms. The solution was simple: face masks, along with other protective devices.
There was an outbreak of disease, but, it turned out, pathogens had nothing to do with it.
Hunting down microbes with planes
"Not many people talk about fungi in chronic disease, except patient groups and I'm sure some you are concerned about fungi”, said Lipkin as he introduced an extraordinary illness where the evidence suggests fungi are to blame.
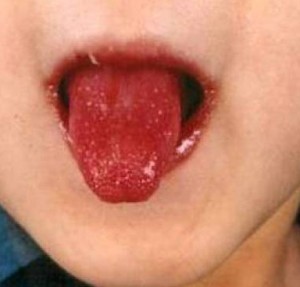
Strawberry tongue and bright red swollen lips are characteristic of Kawasaki disease.
Kawasaki disease occurs suddenly in isolated outbreaks, affects mainly children and was at one time the leading cause of heart disease among Japanese children. It’s named after the Japanese physician who described it in the 1960s and is marked by symptoms including rashes, swollen hands and feet, and ‘strawberry tongue’.
The fundamental problem appears to be inflammation of blood vessels, which in more serious cases affects the heart too. It kills in around 1 per cent of all cases. People have being trying to figure out what causes Kawasaki disease for years, Lipkin’s group included.
Then, a few years ago, a researcher noticed a remarkable association: the outbreaks coincided with changes in wind direction several kilometres up in the atmosphere. Planes with filters flew up to collect samples: they found very little, and most of what they did find was, apparently, methylobacteria.
But it turned out that these bacteria weren’t the answer, just contaminants in the commercial kits they were using to test for microbes (real science is like that). Researchers were rewarded when they cleaned up the contamination: “We went from seventy-three per cent methylobacteria to four per cent. And suddenly we began finding things we had never seen before”, said Lipkin.
Above all they found the fungus Candida, which might yet prove to be the trigger of Kawasaki disease. Intriguingly, a forgotten study from the 1970s showed Candida can cause a Kawasaki-like disease in mice.
Chronic Lyme disease – chasing the wrong microbe?
Fever, fatigue, headaches and a characteristic rash are all characteristic of Lyme disease, which is caused by the bacterium Borrelia burgdorferi and spread through the bites of blood-sucking ticks. It’s treated by antibiotics, but some people remain ill, often leading to the controversial diagnosis of ‘chronic Lyme disease’.
Various theories to explain the illness include prolonged immune activation or even that people are choosing an illness role for secondary gain.
Lipkin is interested in pursuing another theory: what if they’ve got the wrong man and B. burgdorferi isn’t the culprit in some cases? Following the hunch that chronic Lyme disease is caused by a different pathogen, they’ve been looking to see what other microbes are carried by the ticks that spread Lyme disease.
Lipkin said they’ve already discovered a number of different viruses in the ticks. They have more work to do to see if any of these could be causing chronic Lyme disease but added, 'we expect it will surprise many people when it is finally done.'
Autism: from viruses to gene defects and gut bacteria
A new focus of Lipkin’s work is the microbiome, the ecosystems of microbes that colonise our body from gut to mouth to skin. The work began when the CDC asked his laboratory to investigate the possible link between measles RNA from vaccines and children with autism spectrum disorder (ASD) plus gastrointestinal (GI) problems. In blinded studies they found no link, but Lipkin was intrigued by those gut problems.
They compared these ASD/GI children with non-autistic children who had similar gut problems. This work revealed that the ASD children had dramatic reductions in the gene expression of enzymes needed to break down carbohydrates in the gut, as well as of the transport proteins that carry digested carbohydrate across the gut wall.
Lipkin’s team went on to look at the microbiome in the gut and found a relatively obscure bacterium, Sutterella, in the microbiome of around half of patients — but not in controls. What’s more, these patients also produced antibodies against the bacterium Sutterella, suggesting it had penetrated the gut wall and was provoking an immune response.
It’s possible too, said Lipkin, that the bacterium produces some compound that ultimately goes into the brain and causes disease.
These findings might explain why some ASD children respond to antibiotics or changes in diet and probiotics.
Lipkin then highlighted another surprising finding in some of these ASD children with gut problems: a big drop in gene expression of critical detoxifying enzymes. He noted how there had been a big increase in chemicals in the environment in the last hundred years and felt this could well be playing a role in ASD, though as yet there is no firm evidence for it – simply a reduction in detoxifying enzymes.
He went on to say he thought toxins could play a role in ME/CFS too:
With each subset is a disorder that gets diagnosed as ME/CFS.
Microbiome medicine
Lipkin believes the gut and brain could both be important in ME/CFS.
While HIV infection rates are falling in most parts of the world, they continue to rise in Southern Africa, and one of Lipkin’s studies revealed a surprising role of the vaginal microbiome in the spread of HIV.
An anti-retroviral gel helps prevent HIV infection in many women, but some women remain susceptible, and these women have high levels of cytokines in vaginal tissue. Many of them also had high levels of a bacterium called Prevotella in their microbiomes, which was probably driving the high cytokine levels and susceptibility to HIV infection.
Treating these women with antibiotics could reduce their level of Prevotella and cytokines and, in conjunction with the anti-retroviral gel, help protect them from HIV infection.
Brain disorders and immunity
Lipkin is extremely interested in the connection between brain disorders – he includes ME/CFS as one – and immunity, listing a whole set of diseases that have been linked with immune problems including schizophrenia, anorexia and narcolepsy.
And there are a wide range of viruses,bacteria, fungi and parasites implicated in causing these immune problems, such as influenza virus, Borellia bacteria and the toxoplasmosis parasite.
A striking example from his lab is the childhood disorder of tics and obsessive behaviour called PANDAS that is triggered by a simple Streptococcus infection such as ‘strep throat’. Dr. Mady Hornig at Columbia studied this illness using a mouse model. Some clever molecular detective work revealed that antibodies against the strep bacteria were also binding to proteins in the brains of the affected mice, causing the symptoms.
Hornig then found the same thing in the PANDAS children: their antibodies that attacked streptococcus bound to the human equivalent of the mouse brain protein in a test tube (though for obvious reasons the researchers weren’t able to see if the autoantibodies were actually binding in the children’s brain). (Read a fuller explanation of this work.)
Given the link between autoantibodies and brain illness, Lipkin said he was struck by research that found at least some evidence for autoimmunity in ME/CFS, and he thinks it's important they look at this sort of work. He also highlighted the potential for gut microbes to trigger or sustain inflammation or even autoimmunity in illnesses including MS, another reason for doing his ME/CFS microbiome studies.
On the trail of ME/CFS

Mailman School of Pubic Health, where Dr. Lipkin's Center for Infection and Immunity carry out their ME/CFS research.
In a series of illnesses Lipkin has shown how he follows the evidence wherever it leads. And now he has a plan for ME/CFS.
Given his background, the research almost inevitably started with a pathogen hunt, but so far they have drawn a blank.
They used a technique he’d developed called Mass Tag PCR to search for specific pathogens in blood plasma (including enteroviruses, influenza A virus, herpes virus and Borrelia bacteria), but they found no significant differences between patients and controls.
Then, working with Dr. Jose Montoya, Lipkin moved on to high-throughput sequencing that can detect any pathogen, but again they found no specific microbes linked to ME/CFS. They did find that a large but poorly-understood group of viruses - anelloviruses - were less common in patients than controls, but the significance of this is unclear.
The next step is to look in white blood cells (as opposed to plasma), where viruses such as herpes might be hiding out.
Lipkin explained they had profiled cytokines in ME/CFS patients, as had several other groups, but the unpublished results can’t be shared here.
Metabalomics: chemical clues in the blood
Lipkin, like many other researchers, believes the emerging field of metabolomics has the potential to reveal a great deal about diseases. Metabolomics is the study of the complete set of ‘metabolites’, all the small chemicals in any tissue or the blood that result from metabolic processes, such as amino acids or hormones.
Diseases may have particular chemical fingerprints that will give clues about what’s gone wrong in the body, which is why Lipkin is keen to develop his work on this in ME/CFS.
He pointed out that the blood metabolome includes many molecules made by the gut microbiome, as a lot of small molecules cross the gut wall to the blood. For example, some gut bacteria can convert a chemical found in beans and fish into tryptophan, which is actively transported across the gut into the blood. The body needs tryptophan to make the neurotransmitter serotonin.
The gastrointestinal microbiome’s potential to send chemicals into the body is a big reason Lipkin wants to focus on it: 'I think it produces compounds which traffic through the body or into the brain and cause all sorts of curious diseases.'
He added that infection can lead to changes in the microbiome, which could influence the illness. And the microbiome also has the capacity to turn on and turn off the immune system. So the microbiome could be playing a role in ME/CFS in several different ways.
Lipkin is crowdfunding for his microbiome work after twice being turned down by the NIH for strange reasons (reviewers of his application said the illness was either psychosomatic or down to a herpes virus infection in white blood cells).
Lipkin wrapped up by outlining the key ways in which he’s trying to understand ME/CFS. As well as the microbiome and metabolomic work, and cytokine studies in press, he’s planning:
Add these to the completed cytokine study and earlier pathogen hunts and you have a comprehensive programme of research into the possible causes of ME/CFS.
Almost the last thing that Lipkin said in the whole talk really made me sit up as it might explain why he’s investing so much energy in ME/CFS. While Lipkin made his name working on acute infections like SARS and Ebola, he now feels the action is moving to chronic illness:
'I think that the future of microbiology and immunology really rests with understanding microbes and immune responses to microbes and toxicology in chronic diseases ... recently a large focus of our research has been ME/CFS.'
Time for patients to demand action on ME/CFS

Lipkin finished by urging patients to demand that policy makers tackle the problem of ME/CFS. (A recent video highlights that in the last twenty-five years the UK government’s main research bodies have found just £1.6 million for biomedical research.)
Around 1 in 250 people have ME/CFS, which costs the U.S. around $20 billion a year, and probably costs the UK around £4 billion a year, so there are economic as well as compassionate arguments for tackling the illness, said Lipkin.
'You have to be organised and you have to be vocal,' he said – adding that in the U.S. this approach had delivered more research funding for disorders including Alzheimer’s, multiple sclerosis and autism.
Simon McGrath tweets on ME/CFS research:@sjmnotes
The talk Dr. Lipkin gave to patients was very similar to the one he delivered to the CMRC conference the day before and for clarity I occasionally added in some material from that presentation.
Thanks to Russell Fleming for his transcript of the video, which was a huge help in writing this blog.
Photo credits:
Dr. Ian Lipkin
Indian Flying Fox by Dibyendu Ash, Creative Commons CC BY-SA 3.0 licence
Strawberry Tongue via Wikimedia Commons, Creative Commons CC BY 2.0 licence;
Gut & brain image licensed from Canstock.com; Mailman School of Public Health courtesy of The Microbe Discovery Project
Phoenix Rising is a registered 501 c.(3) non profit. We support ME/CFS and NEID patients through rigorous reporting, reliable information, effective advocacy and the provision of online services which empower patients and help them to cope with their isolation.
There are many ways you can help Phoenix Rising to continue its work. If you feel able to offer your time and talent, we could really use some more authors, proof-readers, fundraisers, technicians etc. We’d also love to expand our Board of Directors. So, if you think you can help in any way then please contact Mark through the Forums.
And don’t forget: you can always support our efforts at no cost to yourself as you shop online! To find out more, visit Phoenix Rising’s Donate page by clicking the button below.
 Continue reading the Original Blog Post
Continue reading the Original Blog Post
Hunting down the cause of ME/CFS & other challenging disorders - Lipkin in London
Simon McGrath reports on Dr. Lipkin's talk to patients in London ...
Dr. W. Ian Lipkin
In a talk to patients in London on 3rd September, Dr. W. Ian Lipkin described the extraordinary lengths he and his team are prepared to go to in order to track down the source of an illness, with examples ranging from autism to the strange case of Kawasaki disease.
His talk emphasised the use of high-tech methods and following the evidence wherever it leads, before outlining his ME/CFS research programme that takes a similar approach. And he believes the action in his field is moving from acute illnesses such as SARS to chronic illnesses – including ME/CFS.
Lipkin is a renowned virus hunter who heads up the Center for Infection and Immunity at Columbia University. He’s discovered over 400 viruses, pioneered new molecular techniques for identifying pathogens, and helped the World Health Organisation and Chinese Ministry of Health deal with the SARS outbreak.
You may have seen one of Lipkin's many recent appearances in the media as an expert on Ebola. Yet he now says the future of his field lies not with acute infections, but in understanding the role microbes play in chronic diseases – one reason why ME/CFS has become a major focus his research.
Roll of honour
A lot of people worked together to make possible Dr. Ian Lipkin’s talk to patients on 3rd September in London, as well as the video of it now on YouTube.
A lot of people worked together to make possible Dr. Ian Lipkin’s talk to patients on 3rd September in London, as well as the video of it now on YouTube.
- Dr.. Lipkin is incredibly busy at the moment as an Ebola expert, but still came to the UK both for the CMRC conference and this talk. And he travelled despite breaking his ankle.
- Action for ME organised the talk itself as well as organising and paying for the filming and editing. Its corporate supporter Allen and Overy provided the venue for free.
- The event was hosted with the ME Association who raised the funds to pay for Lipkin’s travel from New York, and accommodation, with many patients donating to bring him to the UK.
- A patient, Sean Kirby, stepped in to clean up the noise on the video soundtrack.
Thank you, one and all.
Proving it
Once upon a time, proving a link between a pathogen and a disease was relatively straightforward. Usually it involved culturing a bug in the lab and showing the bug caused disease in animals too.
But for the most obviously infectious diseases like tuberculosis, smallpox or cholera, the responsible bugs have already been discovered. Lipkin and his team now hunt in more difficult territory, where linking disease with a microbial trigger is altogether more complicated.
We need to find out why people become ill, what sustains the illness and what we can do to mitigate it and prevent it.
Most microbes can’t be cultured in the lab, and often there isn’t an ‘animal model’ of the disease. How, asked Lipkin, would you create a mouse model for brain fog?
So the best way of demonstrating a microbe plays a key role in an illness such as ME/CFS is to show you can treat patients with drugs that target that microbe and that the patients improve or recover – or to find a vaccine that can prevent the illness. No doubt this is just the kind of proof that patients would most appreciate.
Intriguingly, Lipkin first encountered ME/CFS briefly in the 1980s while working as a physician in California, when Dr. Dan Peterson asked him to examine some of his Incline Village patients.
Fast forward to the 1990s and Lipkin had moved into research, and he was asked to investigate a suggested link between Borna disease virus (another virus he’d discovered) and ME/CFS.
He and Birgitta Evengard ran a large study, but found no link with the virus. However, the research did find evidence that ME/CFS patients had immune activation. “I was convinced that this was a biologically based problem, that it was not psychological”. Unfortunately there was no funding then to pursue further research into ME/CFS.
Still, he retained his interest, and when he was asked a few years ago to look at a link between the disease and another virus, this time XMRV/PMLV, he jumped at it. Again the link was disproved for that specific virus, but he’s continuing to hunt for viruses and other bugs as part of his latest programme of ME/CFS research.
Where new human viruses come from

Lipkin et al found 50 new viruses just in the Indian Flying Fox.
Lipkin has probably discovered more viruses than anyone, but he is well aware we’ve only found a fraction of the viral world.
Just how many unknown viruses are out there was highlighted by work Lipkin did as part of the U.S. Agency for International Development’s ‘Predict’ programme, an ambitious effort to find the next Ebola lurking in nature before it spreads out of control.
Most new human viruses start off life in wild mammals, and they often jump to humans via domesticated animals. New forms of flu, for example, often travel into humans from chickens that caught the virus from wild ducks. So one of Predict’s efforts was to estimate how many viruses there were in mammals – and they found a lot.
Taking a single bat species as an example, Lipkin and colleagues found 55 viruses — 50 of which had never been seen before. They detected the viruses from their DNA or RNA using high-throughput sequencing techniques that Lipkin helped pioneer.
Extrapolating from this work and more on other mammals, he and his collaborators conservatively estimated that there are 320,000 different viruses in mammals, most of them unknown.
That’s a pretty big pool of viruses that could produce the next human disease.
Linking Viruses to Human Disease
Some of these unknown viruses may play a role in ME/CFS — we don’t yet know. Showing that a particular virus causes a given disease requires detecting an immune response to the virus, particularly by finding the antibodies that help us fight off an infection.
Looking for antibodies has a huge advantage over looking for microbe DNA or RNA, because antibodies stick around long after the body has defeated the infection and the virus has vanished. Lipkin has previously called this approach of focusing on antibodies as looking for 'shadows of infection', something he’s keen to do in ME/CFS.
Just as there are microarray chips for detecting DNA or RNA of specific viruses, there are now ‘peptide microarrays’ that effectively allow researchers to check for antibodies against any virus. Peptides (i.e., short protein chains) can mimic every possible viral protein that antibodies might bind to.
“You can cover all vertebrate viruses in a single chip, which is amazing”, said Lipkin at the CMRC conference. When blood is run across the peptide-studded chip, the antibodies in the blood glom onto the peptides they’re associated with. And since each antibody was created in response to a particular virus, this reveals the (known) viruses that have ever infected the individual.
Lipkin used this method to great effect to study an outbreak of the MERS virus in the Middle East. He tested camel blood in Saudi Arabia with peptide microarray chips and found that the vast majority had at some point been infected with MERS. Added to other studies, this work showed that camels were the likely cause of the human MERS outbreak in the region.
Some outbreaks of disease are bug-free
It’s important to have an open mind.
In late 2007 a slaughterhouse processing 30 thousand pigs a day reported an outbreak of a neurological disease, and researchers began looking for the pathogen that caused it.
Lipkin and his colleagues realised that the patients worked at or near the section where workers blew brain tissue out of the pig skulls with a high pressure hose, a new technique that had been introduced when plant owners realized there was a market for brain matter in the Far East.
The result was a huge mess, including aerosolized bits of myelin, the fatty insulating sheath around nerve fibres. The workers’ immune systems, it turns out, were reacting hugely to this, triggering the paralysis or weak limbs and other neurological symptoms. The solution was simple: face masks, along with other protective devices.
There was an outbreak of disease, but, it turned out, pathogens had nothing to do with it.
Hunting down microbes with planes
We are open-minded about mechanisms because that’s key, I think.
"Not many people talk about fungi in chronic disease, except patient groups and I'm sure some you are concerned about fungi”, said Lipkin as he introduced an extraordinary illness where the evidence suggests fungi are to blame.
Strawberry tongue and bright red swollen lips are characteristic of Kawasaki disease.
The fundamental problem appears to be inflammation of blood vessels, which in more serious cases affects the heart too. It kills in around 1 per cent of all cases. People have being trying to figure out what causes Kawasaki disease for years, Lipkin’s group included.
Then, a few years ago, a researcher noticed a remarkable association: the outbreaks coincided with changes in wind direction several kilometres up in the atmosphere. Planes with filters flew up to collect samples: they found very little, and most of what they did find was, apparently, methylobacteria.
But it turned out that these bacteria weren’t the answer, just contaminants in the commercial kits they were using to test for microbes (real science is like that). Researchers were rewarded when they cleaned up the contamination: “We went from seventy-three per cent methylobacteria to four per cent. And suddenly we began finding things we had never seen before”, said Lipkin.
Above all they found the fungus Candida, which might yet prove to be the trigger of Kawasaki disease. Intriguingly, a forgotten study from the 1970s showed Candida can cause a Kawasaki-like disease in mice.
Chronic Lyme disease – chasing the wrong microbe?
Fever, fatigue, headaches and a characteristic rash are all characteristic of Lyme disease, which is caused by the bacterium Borrelia burgdorferi and spread through the bites of blood-sucking ticks. It’s treated by antibiotics, but some people remain ill, often leading to the controversial diagnosis of ‘chronic Lyme disease’.
Various theories to explain the illness include prolonged immune activation or even that people are choosing an illness role for secondary gain.
Lipkin is interested in pursuing another theory: what if they’ve got the wrong man and B. burgdorferi isn’t the culprit in some cases? Following the hunch that chronic Lyme disease is caused by a different pathogen, they’ve been looking to see what other microbes are carried by the ticks that spread Lyme disease.
Lipkin said they’ve already discovered a number of different viruses in the ticks. They have more work to do to see if any of these could be causing chronic Lyme disease but added, 'we expect it will surprise many people when it is finally done.'
Autism: from viruses to gene defects and gut bacteria
A new focus of Lipkin’s work is the microbiome, the ecosystems of microbes that colonise our body from gut to mouth to skin. The work began when the CDC asked his laboratory to investigate the possible link between measles RNA from vaccines and children with autism spectrum disorder (ASD) plus gastrointestinal (GI) problems. In blinded studies they found no link, but Lipkin was intrigued by those gut problems.
Some of these kids may have an infection, some may have a genetic defect.
They compared these ASD/GI children with non-autistic children who had similar gut problems. This work revealed that the ASD children had dramatic reductions in the gene expression of enzymes needed to break down carbohydrates in the gut, as well as of the transport proteins that carry digested carbohydrate across the gut wall.
Lipkin’s team went on to look at the microbiome in the gut and found a relatively obscure bacterium, Sutterella, in the microbiome of around half of patients — but not in controls. What’s more, these patients also produced antibodies against the bacterium Sutterella, suggesting it had penetrated the gut wall and was provoking an immune response.
It’s possible too, said Lipkin, that the bacterium produces some compound that ultimately goes into the brain and causes disease.
These findings might explain why some ASD children respond to antibiotics or changes in diet and probiotics.
Lipkin then highlighted another surprising finding in some of these ASD children with gut problems: a big drop in gene expression of critical detoxifying enzymes. He noted how there had been a big increase in chemicals in the environment in the last hundred years and felt this could well be playing a role in ASD, though as yet there is no firm evidence for it – simply a reduction in detoxifying enzymes.
He went on to say he thought toxins could play a role in ME/CFS too:
'My prediction is that you will find a subset that's clearly genetic, a subset that will be microbial, a subset that will be toxic.'
With each subset is a disorder that gets diagnosed as ME/CFS.
Microbiome medicine
Lipkin believes the gut and brain could both be important in ME/CFS.
An anti-retroviral gel helps prevent HIV infection in many women, but some women remain susceptible, and these women have high levels of cytokines in vaginal tissue. Many of them also had high levels of a bacterium called Prevotella in their microbiomes, which was probably driving the high cytokine levels and susceptibility to HIV infection.
Treating these women with antibiotics could reduce their level of Prevotella and cytokines and, in conjunction with the anti-retroviral gel, help protect them from HIV infection.
Brain disorders and immunity
Lipkin is extremely interested in the connection between brain disorders – he includes ME/CFS as one – and immunity, listing a whole set of diseases that have been linked with immune problems including schizophrenia, anorexia and narcolepsy.
And there are a wide range of viruses,bacteria, fungi and parasites implicated in causing these immune problems, such as influenza virus, Borellia bacteria and the toxoplasmosis parasite.
A striking example from his lab is the childhood disorder of tics and obsessive behaviour called PANDAS that is triggered by a simple Streptococcus infection such as ‘strep throat’. Dr. Mady Hornig at Columbia studied this illness using a mouse model. Some clever molecular detective work revealed that antibodies against the strep bacteria were also binding to proteins in the brains of the affected mice, causing the symptoms.
Hornig then found the same thing in the PANDAS children: their antibodies that attacked streptococcus bound to the human equivalent of the mouse brain protein in a test tube (though for obvious reasons the researchers weren’t able to see if the autoantibodies were actually binding in the children’s brain). (Read a fuller explanation of this work.)
Given the link between autoantibodies and brain illness, Lipkin said he was struck by research that found at least some evidence for autoimmunity in ME/CFS, and he thinks it's important they look at this sort of work. He also highlighted the potential for gut microbes to trigger or sustain inflammation or even autoimmunity in illnesses including MS, another reason for doing his ME/CFS microbiome studies.
On the trail of ME/CFS
Mailman School of Pubic Health, where Dr. Lipkin's Center for Infection and Immunity carry out their ME/CFS research.
In a series of illnesses Lipkin has shown how he follows the evidence wherever it leads. And now he has a plan for ME/CFS.
Given his background, the research almost inevitably started with a pathogen hunt, but so far they have drawn a blank.
They used a technique he’d developed called Mass Tag PCR to search for specific pathogens in blood plasma (including enteroviruses, influenza A virus, herpes virus and Borrelia bacteria), but they found no significant differences between patients and controls.
Then, working with Dr. Jose Montoya, Lipkin moved on to high-throughput sequencing that can detect any pathogen, but again they found no specific microbes linked to ME/CFS. They did find that a large but poorly-understood group of viruses - anelloviruses - were less common in patients than controls, but the significance of this is unclear.
The next step is to look in white blood cells (as opposed to plasma), where viruses such as herpes might be hiding out.
Lipkin explained they had profiled cytokines in ME/CFS patients, as had several other groups, but the unpublished results can’t be shared here.
Metabalomics: chemical clues in the blood
Lipkin, like many other researchers, believes the emerging field of metabolomics has the potential to reveal a great deal about diseases. Metabolomics is the study of the complete set of ‘metabolites’, all the small chemicals in any tissue or the blood that result from metabolic processes, such as amino acids or hormones.
Diseases may have particular chemical fingerprints that will give clues about what’s gone wrong in the body, which is why Lipkin is keen to develop his work on this in ME/CFS.
He pointed out that the blood metabolome includes many molecules made by the gut microbiome, as a lot of small molecules cross the gut wall to the blood. For example, some gut bacteria can convert a chemical found in beans and fish into tryptophan, which is actively transported across the gut into the blood. The body needs tryptophan to make the neurotransmitter serotonin.
The gastrointestinal microbiome’s potential to send chemicals into the body is a big reason Lipkin wants to focus on it: 'I think it produces compounds which traffic through the body or into the brain and cause all sorts of curious diseases.'
He added that infection can lead to changes in the microbiome, which could influence the illness. And the microbiome also has the capacity to turn on and turn off the immune system. So the microbiome could be playing a role in ME/CFS in several different ways.
Lipkin is crowdfunding for his microbiome work after twice being turned down by the NIH for strange reasons (reviewers of his application said the illness was either psychosomatic or down to a herpes virus infection in white blood cells).
Lipkin wrapped up by outlining the key ways in which he’s trying to understand ME/CFS. As well as the microbiome and metabolomic work, and cytokine studies in press, he’s planning:
- Further pathogens searches, this time in white blood cells (where herpes viruses, for instance, can hide out).
- Gene expression studies to see if patients have different genes active to healthy controls, which could help show what’s going wrong
- Proteomics, which is the ‘protein fingerprint’ of the blood much like metabolomics is the chemical fingerprint. Again, differences between patients and controls might reveal clues about what’s going wrong in the illness.
- Functional Immunology with the National Institute of Allergies and Infectious Diseases.
Add these to the completed cytokine study and earlier pathogen hunts and you have a comprehensive programme of research into the possible causes of ME/CFS.
Almost the last thing that Lipkin said in the whole talk really made me sit up as it might explain why he’s investing so much energy in ME/CFS. While Lipkin made his name working on acute infections like SARS and Ebola, he now feels the action is moving to chronic illness:
'I think that the future of microbiology and immunology really rests with understanding microbes and immune responses to microbes and toxicology in chronic diseases ... recently a large focus of our research has been ME/CFS.'
Time for patients to demand action on ME/CFS
Lipkin finished by urging patients to demand that policy makers tackle the problem of ME/CFS. (A recent video highlights that in the last twenty-five years the UK government’s main research bodies have found just £1.6 million for biomedical research.)
Around 1 in 250 people have ME/CFS, which costs the U.S. around $20 billion a year, and probably costs the UK around £4 billion a year, so there are economic as well as compassionate arguments for tackling the illness, said Lipkin.
'You have to be organised and you have to be vocal,' he said – adding that in the U.S. this approach had delivered more research funding for disorders including Alzheimer’s, multiple sclerosis and autism.
Simon McGrath tweets on ME/CFS research:@sjmnotes
The talk Dr. Lipkin gave to patients was very similar to the one he delivered to the CMRC conference the day before and for clarity I occasionally added in some material from that presentation.
Thanks to Russell Fleming for his transcript of the video, which was a huge help in writing this blog.
Photo credits:
Dr. Ian Lipkin
Indian Flying Fox by Dibyendu Ash, Creative Commons CC BY-SA 3.0 licence
Strawberry Tongue via Wikimedia Commons, Creative Commons CC BY 2.0 licence;
Gut & brain image licensed from Canstock.com; Mailman School of Public Health courtesy of The Microbe Discovery Project
Phoenix Rising is a registered 501 c.(3) non profit. We support ME/CFS and NEID patients through rigorous reporting, reliable information, effective advocacy and the provision of online services which empower patients and help them to cope with their isolation.
There are many ways you can help Phoenix Rising to continue its work. If you feel able to offer your time and talent, we could really use some more authors, proof-readers, fundraisers, technicians etc. We’d also love to expand our Board of Directors. So, if you think you can help in any way then please contact Mark through the Forums.
And don’t forget: you can always support our efforts at no cost to yourself as you shop online! To find out more, visit Phoenix Rising’s Donate page by clicking the button below.
Last edited:
