

Doctors with ME Confront the Taboo of Suicide
Eleanor Stein, MD and Lily Chu, MD are both doctors with myalgic encephalomyelitis (ME). They have dedicated their careers to helping others with ME. Images courtesy of Dr. Eleanor Stein and Dr. Lily Chu.
By Bronc
It was a warm summer evening and I was looking forward to watching one of my favourite films, when I received a text from my best friend.
I expected the text to be a question asking me what film I was going to watch. Instead, he informed me that the night before he had attempted to kill himself.
The next day, when we met, he explained that he could not endure his suffering anymore and that is why he made the suicide attempt. Now my dear friend, whom I loved as a brother, was just one amongst many other tragic stories.
There is plenty of evidence to suggest that there are several communities who are at much higher risk of suicide than the rest of the general population.
My dear friend belonged to one of those highly vulnerable groups.
There is also a body of evidence to suggest that people with myalgic encephalomyelitis (ME) are one of those highly vulnerable groups. For example, in the UK, people with ME have a more than six-fold increase in suicide risk compared to the general population.
Last year I spoke with Professor Leonard Jason and Madeline Johnson about the risk factors for suicide amongst people with ME.
More recently, I caught up with Dr. Lily Chu and Dr. Eleanor Stein to discuss their publication on suicide prevention strategies for people with ME, entitled “Identifying and Managing Suicidality in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome.” Co-authors Leonard Jason and Ms. Meghan Elliott also contributed to the conversation.

"In 2006 I came down with ME/CFS. I was surprised by how little we knew about it medically and scientifically, as well as by how challenging it was to find physicians specializing in this condition. The amount of prejudice and misconceptions among medical and scientific professionals was astounding."
—Lily Chu, MD
Phoenix Rising:
How did you get involved in the field of ME/CFS research?
Dr. Eleanor Stein:
I became an ME clinician due to my own illness experience. Becoming ill in 1989, before much was known, I had to do my own research to regain the ability to function and work. Then, when I had the opportunity, I decided to go into the field to keep learning and share my knowledge with patients so they wouldn’t have to work as hard as I did to learn about ME.
Dr. Lily Chu:
Originally, I worked as an internal and geriatric medicine physician taking care of elderly people. My research involved examining the quality of medical care in nursing homes. In 2006 I came down with ME/CFS.
I was surprised by how little we knew about it medically and scientifically, as well as by how challenging it was to find physicians specializing in this condition. The amount of prejudice and misconceptions among medical and scientific professionals was astounding.
I thought I could apply my skills and experience to advance this field, to help myself and other people who were sick.
I became interested in this particular topic because I knew several people affected by ME/CFS who had died by suicide. They were in their 30s and 40s and had led vibrant lives. There were many things they wanted to do but they found day-to-day living very difficult. I had taken care of patients at risk for suicide before but they were different from this group.
"My patients still routinely hear from health care professionals that there is nothing wrong with them. I heard it from more than one patient TODAY."
—Eleanor Stein, MD
Phoenix Rising:
Multiple studies have found that adults suffering from ME/CFS are at a heightened risk of death by suicide. For example, here in the United Kingdom, people with ME/CFS have a more than six-fold increase in suicide risk compared to the general population.
Despite this risk being a clear and urgent public health issue, there is no mention of it in the new ME/CFS guidelines that were issued by the UK National Institute of Clinical Excellence (NICE) back in October 2021.
Why do you think that public health authorities have done so little to address this issue?
Dr. Eleanor Stein:
The [notable absence] of the increased suicide risk in people with ME in treatment guidelines is in keeping with the overall lack of attention to, and validation of, ME as a serious health condition. My patients still routinely hear from health care professionals that there is nothing wrong with them. I heard it from more than one patient TODAY.
As chair of a working group of ICanCME — a Canadian research team funded by the Canadian Institutes of Health Research (CIHR) — I am involved in research to identify gaps and barriers to care and then to design a model of care that will better meet the needs of Canadians with ME.
Dr. Lily Chu:
I don’t know for certain why NICE and public health authorities have not addressed this topic in depth. There are probably many reasons, some specific to ME/CFS and some not:
One:
In the USA, because we do not have a national healthcare or medical record system, it is difficult to access data and actively surveil for healthcare trends — whether the condition in question is heart disease, diabetes, depression, suicide or ME/CFS.
Two:
The content of death certificates greatly influence the data available. Historically, up to 91% of people with ME/CFS have not been diagnosed or have been misdiagnosed. As Dr. Stein stated, some healthcare professionals still do not view ME/CFS as a legitimate medical condition.
[Any undiagnosed patients] will not have ME/CFS listed on their death certificate. Even if [a patient is correctly] diagnosed, there are no rules mandating which or how many conditions clinicians must list as contributing factors. Individuals and families may also have preferences about which conditions are included.
Thus, someone might have suicide listed on their death certificate, but not ME/CFS. [These realities] make it hard to track suicide and ME/CFS. I also wonder about the accurate identification of suicides in general. For example, some deaths may be misclassified as accidents (e.g. unintentional overdosing of a drug) — when in fact the person died by suicide.
Three:
We need more — and more rigorous — studies replicating or supporting the increased risk of suicide. We cited several studies in our recent paper showing an increased risk of suicide among people with ME/CFS compared to the general population.
However, at least one study found that the suicide rate is higher for people affected by [general] chronic fatigue, but not [for people affected] by chronic fatigue syndrome. The study’s methods or results can be debated but it has likely influenced researchers in the past.
In general, the more studies showing an increased risk, the more likely authorities are to respond. For example, the field would benefit from prospective, longitudinal studies and studies based on state-, regional-, and national-level data.
Four:
The squeaky wheel gets the grease. There are often more demands placed on public health authorities than they have staff, funding and resources to respond with. Thus, it is not surprising that they tend to address issues that are in the news, brought up to them by their superiors, are deemed important by their staff, etc.
If people with ME/CFS want more attention focused on this topic, I would encourage them to contact their government representatives and local public health agencies.
"Each time someone with ME takes their life, it is a failure of the medical system. No one should feel that suicide or [Medical Assistance in Dying] are their only options."
—Eleanor Stein, MD
Phoenix Rising:
Can you explain some of the socio-economic and medically-related risk factors for suicide facing people with ME/CFS?
Dr. Eleanor Stein:
Over the past 22 years during which I have devoted my practice to ME, several of my patients have committed suicide and at least one that I know of has died by Medical Assistance in Dying (MAiD).
In every case, these individuals had some combination of poverty, social isolation, perceived lack of medical support and unremitting, unbearable symptoms — including post-exertional malaise, sensitivities, pain, disturbed sleep, cognitive dysfunction and severe-to-extreme disability.
If any of those facets of their experience had been addressed, especially the severe symptoms, I suspect many would not have chosen suicide. Each time someone with ME takes their life, it is a failure of the medical system.
No one should feel that suicide or MAiD are their only options. Their [situation] should activate a comprehensive intervention to identify and remedy the things that are making life unbearable.
" 'Thwarted belongingness' (a technical term describing the feeling of not fitting in anywhere) and unsupportive social interactions can be experienced by anyone with a chronic illness. However, people with ME/CFS might encounter them to a greater degree."
—Lily Chu, MD
Dr. Lily Chu:
As Dr. Stein mentions, people with ME/CFS frequently experience a combination of factors that put them at risk. Table 1 in our paper [reproduced below] lists these factors.
Most likely do not need to be explained to Phoenix Rising readers. Some factors, though, might be more common or severe due to the nature of ME/CFS and the lack of knowledge about this condition among the public.
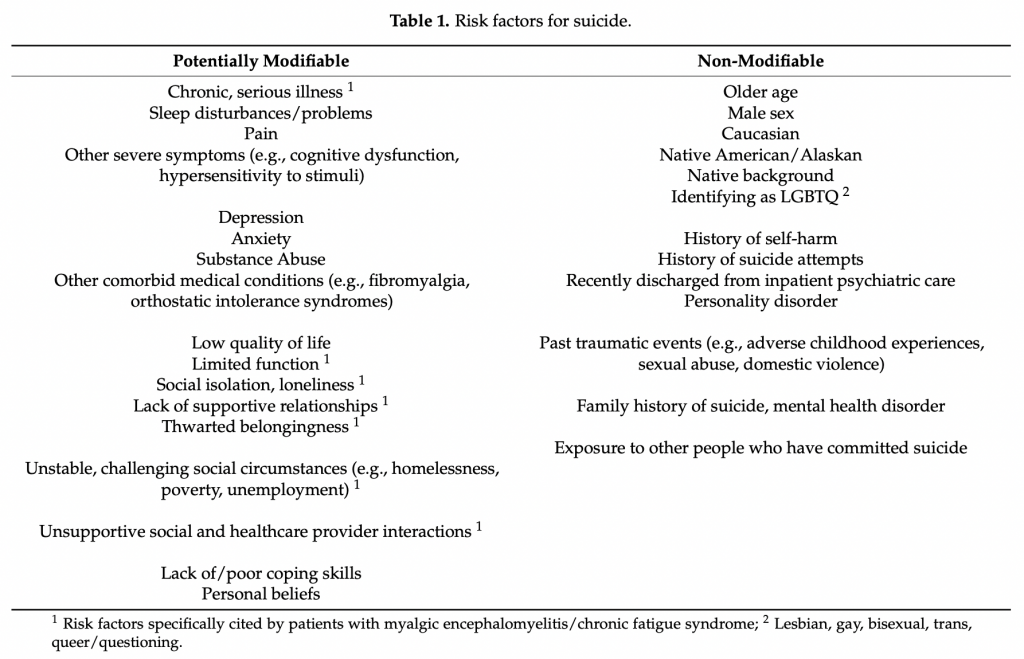
For example, (Ahmedhani et al., 2017) found that among people who committed suicide, almost 20% were diagnosed with a sleep disorder. One major ME/CFS symptom is unrefreshing sleep. Decreased ability to function — at work, school, or in the home — and feeling like a burden to others are known to be associated with suicide.
About a quarter of people with ME/CFS are home- or bed-bound and even those who are not [home- or bed-bound] often cannot work or go to school. Some people with ME/CFS feel sad and guilty about having to depend on their aging parents for personal care tasks like dressing or bathing.
Interestingly, my co-authors Dr. Leonard Jason and Ms. Megan Elliot found that people who are home-bound are the most at risk.
One reason [for this finding] may be [the fact that] bed-bound patients are so severely affected that they might not have the capacity to harm themselves. This is similar to what has been observed with depression, [where] the riskiest time is when the depression has just started to lift.
“Thwarted belongingness” (a technical term describing the feeling of not fitting in anywhere) and unsupportive social interactions can be experienced by anyone with a chronic illness. However, people with ME/CFS might encounter them to a greater degree.
Lack of understanding from healthcare providers, being labelled as “rebellious” or “noncompliant” because they disagreed with now-disproven treatments, being blamed for their own illness, and the burden of having to educate others have led to suicidal feelings, depression, and hopelessness among ME/CFS patients both in the United States and in Spain.
Many of these factors are potentially modifiable. Some people, including healthcare professionals, believe prevention of suicides is impossible.
By breaking down a seemingly difficult problem into smaller parts, I hope we can show clinicians that addressing each part might resolve or reduce suicidality for individual patients.
"The notion that all or most suicides are linked to depression has been questioned in recent years. […] I was surprised to learn that only recently have researchers started to directly seek the perspectives of people who have attempted or survived suicide."
—Lily Chu, MD
Phoenix Rising:
Why do you think some people with ME/CFS who are experiencing suicidal thoughts may be reluctant to engage with mental health care services?
Dr. Eleanor Stein:
People are reluctant to tell health care professionals about suicidal thoughts because of their experience that doing so leads providers to assume they are depressed.
Many fear involuntary hospitalization and recommendations such as psychotropic medication, CBT, exercise, and activation therapy — treatments that are at best ineffective and at worse harmful for people with severe ME.
Dr. Lily Chu:
I agree with Dr. Stein. For many years, healthcare professionals believed ME/CFS to be a form of depression, anxiety, or other psychological or psychiatric illness. Unfortunately, those beliefs still exist in some circles. Thus, some people with ME/CFS are afraid that they will be misdiagnosed with depression.
Another group may actually suffer from clinical depression. This is not unexpected due to the challenges forced upon anyone with a serious illness. It is vital, though, that healthcare workers recognize that depression and anxiety are not symptoms of ME/CFS itself.
In [any case], given what has happened in the past, people are justifiably concerned that their ME/CFS symptoms will be erroneously attributed to depression or another psychiatric condition. Subsequently, [they are concerned that] they might be prescribed medications, psychological treatments, and/or physical activities which might worsen their symptoms.
In our recent paper, we also emphasize that suicidal thoughts and behaviors can occur in the absence of depression. The notion that all or most suicides are linked to depression has been questioned in recent years.
In the past, researchers often interviewed friends and relatives after a person had died by suicide. In some cases, the diagnosis of depression was made retrospectively and so might not be accurate. I was surprised to learn that only recently have researchers started to directly seek the perspectives of people who have attempted or survived suicide.
Some people may also feel that seeking care is futile, that nothing much can be done to help them. But there are many actions they and their healthcare providers can take. Besides treatment for depression, steps like constructing a suicide safety plan, addressing uncontrolled symptoms, or obtaining assistive devices can reduce suicidality by increasing a person’s quality of life or function.
"I once attended a webinar given by a former [disability benefits examiner] who told the doctors present that their supportive documentation could literally save lives. He had had a few clients die after their benefits were denied."
—Lily Chu, MD
Phoenix Rising:
In the research paper that you co-authored last year, Identifying and Managing Suicidality in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome, you and your colleagues outline a strategy for assessing suicidality in people with ME/CFS. Can you explain this strategy?
Dr. Lily Chu:
Our strategy is outlined in Figure 1 of the paper, [reproduced below], and is meant for medical providers who are not mental health professionals working in an outpatient (clinic) setting. Studies of completed suicides show that 50% of people visited their medical provider in the prior month. In contrast, only 30% had seen a mental health professional in the year prior.
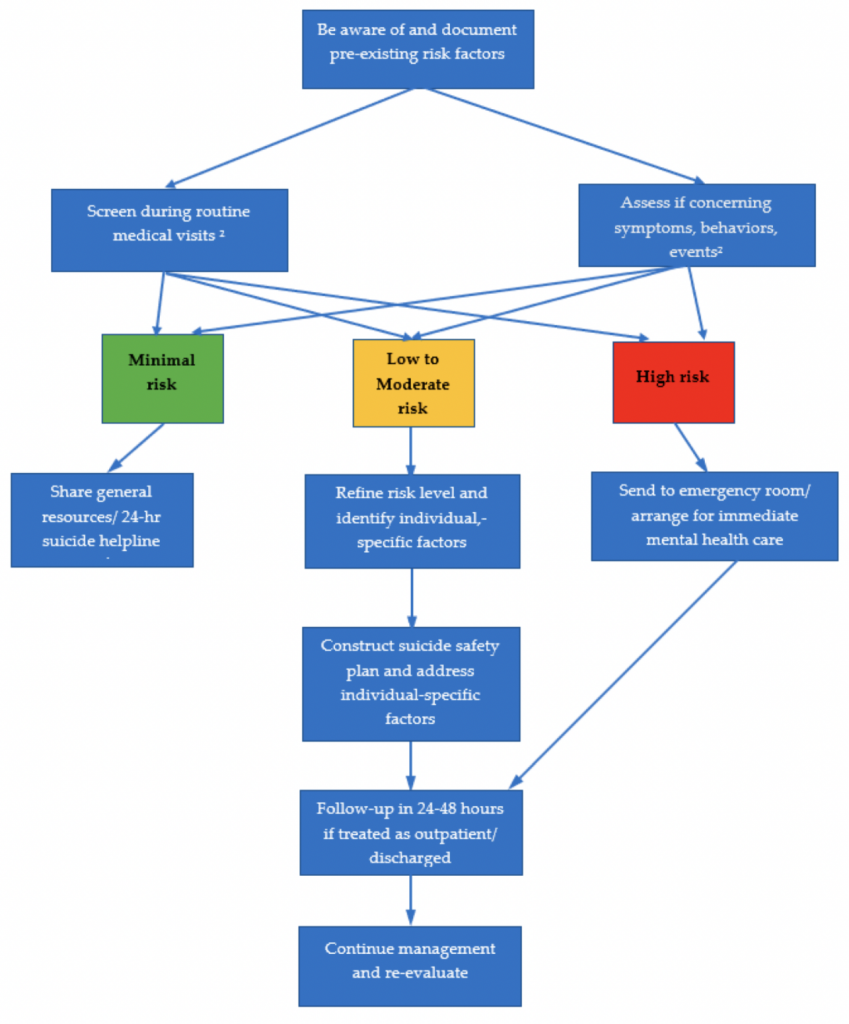
Our approach consists of a few steps:
One: Medical professionals should decide whether they wish to ask all patients about suicide (universal screening) OR ask only those patients who show concerning behaviors (selective screening).
Universal screening is controversial because it may not identify more people at risk or reduce suicidality.
[For selective screening, we list in Table 2] examples of concerning statements (“My family would be better off if I were dead.”), symptoms (e.g. sadness, irritability), behaviors (e.g. stopping enjoyable hobbies), and events (e.g. unemployment, denial of benefits).
Two: [Medical professionals should] screen patients using the Columbia-Suicide Severity Scale or the Ask Suicide-Screening Questionnaire (Figures 3 and 2, respectively).
These were developed, respectively, by Columbia University in New York and by the US National Institutes of Health. Medical professionals often report that they don’t know how to ask about suicide, so these questionnaires are meant to help.
They serve two purposes: 1) to separate suicidal from non-suicidal patients and 2) if a patient is suicidal, to help professionals determine their level of risk (low, moderate, high). The level of risk affects how quickly care needs to be initiated and what setting might be best (e.g. hospital or clinic).
As mentioned earlier, people with ME/CFS are often afraid that they will be hospitalized against their will. At least in the US, the standard for psychiatric care is to choose the least restrictive setting where the individual can still be safe. Thus, hospitalization is not often the first choice.
People affected by both ME/CFS and a psychiatric illness may also want to complete a psychiatric advance directive, which allows patients early and increased input into their own care.
For example, an individual might state that cognitive behavioral therapy (CBT) is acceptable for treating their depression but not [for treating] their ME/CFS-related symptoms. They can then list which of their symptoms [stem] from depression [and which of their symptoms stem from] ME/CFS.
Three: [Medical professionals should] refine the risk level for patients deemed to be at low or moderate risk.
Patients who are at no risk or at minimal risk don’t need further action and those [who turn out to be] at high risk should be referred for immediate psychiatric care.
Medical professionals should review risk and protective factors (Table 1 and Table 3) for each individual to confirm that they are indeed low or moderate risk. Going through the factors will also help them plan treatment.
Four: [Medical professionals should] create a treatment plan that incorporates best practices for all patients at risk of suicide as well as interventions tailored to the individual patient (Table 5).
Examples of the former would include evaluating for and treating depression, and instructing patients how to create a suicide safety plan (Table 4). Examples of the latter might include sleep medications, pain management, assessment for a wheelchair, supportive letters for accommodations and benefits, etc.
Tangentially, I once attended a webinar given by a former Social Security Disability Insurance (SSDI) employee who told the doctors present that their supportive documentation could literally save lives. He had had a few clients die after their benefits were denied.
My co-author Megan Elliott notes that suicide safety plans may still be helpful for individuals even if not completed with a healthcare professional. I would suggest making a copy and sharing it with a trusted family member or friend. They can help carry out or reinforce certain steps. Here are instructions and a form to use.
Five: [Medical professionals should] plan to follow-up regularly with the patient.
This follow-up can be done by the healthcare provider or by their staff members. Something simple, like one or two short telephone calls or e-mails, can support the patient emotionally and also inform the provider as to whether the treatment plan needs to be adjusted [between in-person] appointments.
"People with ME become suicidal when their suffering is unbearable and their attempts to get their […] needs met have been unsuccessful. When asked, most patients tell me what would help them feel that life would be worth living. It is not rocket science."
—Eleanor Stein, MD
Phoenix Rising:
How can public health authorities best manage at-risk patients in an outpatient setting?
Dr. Eleanor Stein:
People with ME become suicidal when their suffering is unbearable and their attempts to get their financial, social, home care and medical needs met have been unsuccessful. When asked, most patients tell me what would help them feel that life would be worth living. It is not rocket science.
Ask the patient what they need and provide it. This requires the providers and the system to believe what patients tell them and to work to find the needed resources.
Dr. Lily Chu:
Our recent paper primarily targeted individual healthcare professionals and [outlined] what they could do. For many people affected by suicidal thoughts, the first person or group they reach out to is usually their regular medical provider or clinic.
[Neither I nor my co-authors have worked in] or led public health agencies. Thus, we did not go into detail about what these organizations can or should do.
Some possible roles [for public health authorities] include education, direct service, and epidemiological research.
[Government] agencies can make the public aware of the warning symptoms or signs [of suicidality], the services available locally, and the actions people can take to help loved ones.
Authorities can update local healthcare providers and organizations about best practices and about how to refer people to local programs. Many physicians readily admit that they are not well trained with regard to managing suicidality.
“Direct service” could mean operating a free or low-cost mental health clinic, running support groups, or maintaining telephone hotlines. Assessing and monitoring rates of suicide in the local area is one example of research.
Regarding ME/CFS, public health authorities could disseminate accurate information and [work to] correct misconceptions about this disease. This could be [accomplished with] something as simple as a webpage about ME/CFS or by mentioning ME/CFS in the context of chronic illness as a risk factor for suicide.
[Such efforts] might improve how healthcare professionals react when a person with ME/CFS shows up in their practice clinically depressed or expressing suicidal thoughts.
In 2019 Dr. Jason, Dr. Jose Montoya and I gave a virtual presentation to the US National Suicide Prevention Lifeline about ME/CFS. However, a one-time presentation is not enough to be comprehensive or to ensure that the information sticks [with the audience].
"Many of the risk factors that we outline in our paper — like joblessness, poverty, social isolation — are social consequences of chronic illness but are not medical issues in and of themselves. Short of a cure or a treatment that restores near-normal health, the solutions to these issues must be social ones."
—Lily Chu, MD
Phoenix Rising:
Reducing risk factors for suicide in people with ME/CFS requires more than just a medical approach. What could government, both local and national, do to help reduce the risk of suicide?
Dr. Lily Chu:
I agree that we need more than just a medical approach. Many of the risk factors that we outline in our paper — like joblessness, poverty, social isolation — are social consequences of chronic illness but are not medical issues in and of themselves. Short of a cure or a treatment that restores near-normal health, the solutions to these issues must be social ones.
At the end of our paper, we cite one essay discussing how increasing the minimum wage can decrease suicide rates. Similarly, simple “check-ins” (e.g. short e-mails, phone calls, or texts twice a week by volunteers) have been shown to reduce risk.
Although not in our paper, [the US food delivery charity] Meals on Wheels not only provides food to home-bound seniors but also has been shown to decrease loneliness. In retrospect these types of efforts seem obvious, but studying and isolating the effect of such interventions can be difficult. I’m really looking forward to more research in this area.
Our paper targeted individual clinicians, but most are not in a position to make such changes or start such programs on their own. However, they can find and connect their patients to any available community-based programs and they can also supply any documentation needed to qualify them for services.
I cited [the case of] Meals on Wheels earlier. Some [Meals on Wheels locations] supply meals to disabled, home-bound, younger people. However, clinicians must complete paperwork verifying the need for such services. [Such paperwork] is especially vital for a condition like ME/CFS that the general public is less familiar with.
"There are many gaps in, and limits to, what we know currently — both about suicidality in general and about ME/CFS in particular. […] In 2011, the UK think-tank Demos made headlines when they found that approximately 10% of suicides are linked to chronic or terminal physical illness and not necessarily to a mental illness."
—Lily Chu, MD
Phoenix Rising:
What further research do you believe is needed into this important public health issue?
Dr. Eleanor Stein:
[We need] a study of pragmatic holistic care to meet the needs of the severely ill. (e.g. providing finances, stable home care, empathic and effective symptom management, home-based care, etc.)
Dr. Lily Chu:
There are many gaps in, and limits to, what we know currently — both about suicidality in general and about ME/CFS in particular. Here are some areas that I feel would benefit from research.
One: Diagnosis and care of suicidal patients in an outpatient setting by medical — not mental health — professionals.
Most research has taken place in settings where the staff specialize in psychiatric or psychological care (e.g. mental health clinics, psychiatric hospitals). Yet the great majority of people struggling with suicidal thoughts or behaviors don’t seek out or have access to mental health care.
If they do talk to anyone, it’s commonly to their primary care physician or provider. Furthermore, most patients likely do not need nor desire to be hospitalized.
Two: Suicidal thoughts or behaviors among terminally or chronically ill patients.
Most healthcare professionals sense that these patients are at high risk for suicide. Yet, the research focusing on this group is sparse. In 2011, the UK think-tank Demos made headlines when they found that approximately 10% of suicides are linked to chronic or terminal physical illness and not necessarily to a mental illness.
The reasons why chronically ill people consider suicide and the solutions to prevent them from acting on their thoughts might be very different from those [reasons and solutions] involving physically healthy people.
I know of several situations where people have died by suicide or considered it, yet they did not consider themselves depressed. Instead, as noted earlier, factors like severe symptoms, decreased function, poverty, etc. played a bigger role.
Three: Embedding psychiatric care in primary care clinics.
It is neither realistic nor optimal [to have] medical providers who are not experts in mental healthcare manage all [types of] patients. Patients can fall through the cracks when they need to travel to another place at another time for specialty care.
Some organizations are experimenting with medical clinics that include a psychiatrist, psychiatric nurse, or similar person on site. They can easily advise their colleagues and see patients urgently if needed.
Four: Effectiveness and feasibility of remote delivery of mental healthcare.
The COVID-19 pandemic forced many healthcare professionals and organizations to look into alternative healthcare delivery models. Remote and/or asynchronous mental healthcare — delivered via e-mail, telephone, or video conferencing software — already exists but its availability has been limited.
People with severe depression who cannot leave their homes, people living in rural areas, and those who need close monitoring would benefit from such services. At the same time, we know that about a quarter of ME/CFS patients are home- or bed-bound, so progress in this area would also help people with ME/CFS.
Five: Research focusing on suicide and ME/CFS.
As I mentioned earlier, we need more and better data. For example, I have thought about designing a study to examine how common suicidal thoughts, behaviors, and attempts are among people with ME/CFS. [This study] could also check whether the reasons behind suicidality observed earlier by Dr. Jason’s group can be replicated.
Besides the usual logistical and funding issues, one major concern I have [with such a study] is how to handle study participants recognized to be at moderate or high risk for suicide. It would be unethical to identify these individuals, yet not take action to help them.
(If anyone is interested in funding or helping me to organize such a study, please contact me via iacfsmeorg@gmail.com)
As Dr. Stein stated, trials looking at what interventions might help are also urgently needed.
If you or a loved one is feeling suicidal and you are in the USA, please call the National Suicide Prevention Helpline at 1-800-273-8255.
If you are in Canada, call the Canada Suicide Prevention Service at 1-833-456-4566.
If you are in another country, see this list of international helplines.
For more information about suicide, including what might happen when you call for help, see this Helpguide webpage.
Bronc is a former historian who is active in his local ME support group. He enjoys interviewing scientists involved in ME research to help himself and others better understand their illness.
Acknowledgment: The author would like to thank Jody Smith and Eric Pyrrhus for help with editing and preparing this article.
Last edited by a moderator:


 ”
”