
Dx Revision Watch
Suzy Chapman Owner of Dx Revision Watch
- Messages
- 3,061
- Location
- UK
...Nice find!
I'll check the page from time to time to see whether the
"Preliminary programme and List of Participants"
is made available.
Suzy

...Nice find!
Hi Suzy,
Very good - and I like your new "blurb" above your rag doll image: ME agenda's sites are to be highly recommended to anyone interested in ME and the institutions and persons concerned with it.
Chamfort:
"Presque tous les hommes sont esclaves, par la raison que les Spartiates donnaient de la servitude des Perses, faute de savoir prononcer la syllabe non. Savoir prononcer ce mot et savoir vivre seul sont les deux seuls moyens de conserver sa libert et son charactre."
I may have found a new signature."Take smoking and lung cancer. People think of it as a physical illness but lung cancer is a behaviour disease due to smoking habit."
I was wrong. This is the stupidest thing I have ever read
"Take smoking and lung cancer. People think of it as a physical illness but lung cancer is a behaviour disease due to smoking habit."
(Btw Suzy: about your avatar blurb.. "hellion" will fit...)
I was wrong. This is the stupidest thing I have ever read:
I may have found a new signature.
(Btw Suzy: about your avatar blurb.. "hellion" will fit...)
I cannot think of higher praise, nor someone more worthy of it. :Retro wink:
I was wrong. This is the stupidest thing I have ever read:
I may have found a new signature.
(Btw Suzy: about your avatar blurb.. "hellion" will fit...)
Also note the conflation of 'mind' and 'brain' in the writing, as if they were the same thing...
Dr. Yes says:
I was wrong. This is the stupidest thing I have ever read.
Angela Kennedy says:
Also note the conflation of 'mind' and 'brain' in the writing, as if they were the same thing...
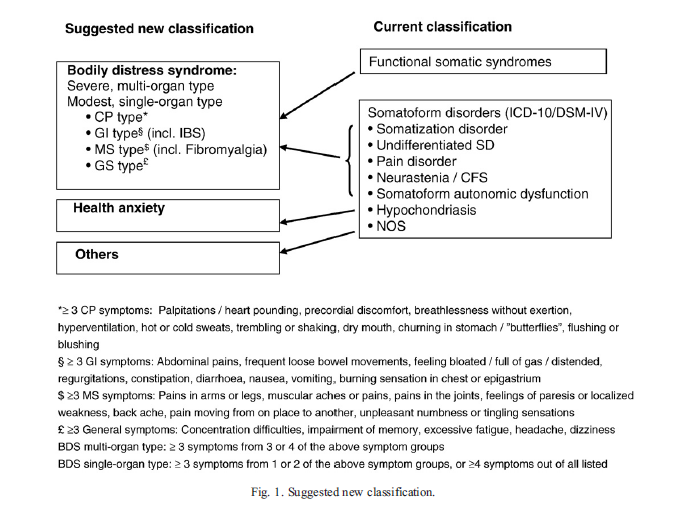
"Finally, the bodily distress syndrome diagnosis
may have the potential to facilitate patient care given that
very similar treatments have been shown to be effective in
various functional somatic syndromes [47-51] and
somatoform disorders [19,52,53]. It may be easier to
deliver these treatments if patients currently receiving
various diagnostic labels are given the same diagnosis."
- Musculoskeletal symptoms subtype [Pains in arms or legs (2.014), Muscular
aches and pains (2.013), Pains in the joints (2.015), Feelings of paresis or
localized weakness (2.055), Back ache (2.012), Pain moving (2.023),
Unpleasant numbness or tingling sensations (2.058)]
- General symptoms subtype [Concentration difficulties (7.001), Impairment
of memory (2.066), Excessive fatigue (2.087 OR 2.088), Headache (2.010),
Dizziness (2.063)]
- Gastrointestinal symptoms subtype [Abdominal pains (2.017), Frequent loose
bowel movements (2.029), Feeling bloated/full of gas/distended (2.027),
Regurgitations (2.026), Constipation (2.028), Diarrhea (2.030),
Nausea (2.024), Vomiting (2.025), Burning sensation in chest or epigastrium
(2.034)]
- Cardiopulmonary symptoms subtype [Palpitations/heart pounding (2.037 OR
2.074), Precordial discomfort (2.038), Breathlessness without exertion
(2.039), Hyperventilation (2.041), Hot or cold sweats (2.075),
Trembling or shaking (2.076), Dry mouth (2.077), Churning in
stomach/"butterflies" (2.079), Flushing or blushing (2.078)]
1.self-reported impairment in short-term memory or concentration severe enough to cause substantial reduction in previous levels of occupational, educational, social, or personal activities;
2.sore throat;
3.tender cervical or axillary lymph nodes;
4.muscle pain;
5.multi-joint pain without joint swelling or redness;
6.headaches of a new type, pattern, or severity;
7.unrefreshing sleep;
8.post-exertional malaise lasting more than 24 hours.
You flatlanders amaze me with your hand wrapped around your brain like that and clicking you boots and uttering your heil slogans to the gods of good science but then you turn around and unravel and offer yourselves up to the gods of psychobabble.
These gods offer up a pot fermented in the juices of Freudian, Jungian, a dash of Rogerian, a little dash of Gestalt but finding the stew lacking some meat, these gods throw in a bunch of frontal lobotomies from years past and zap it with some good old electric shock therapy. Finding it lacking in some kick, they spice it up with some pop psych, "I'm OK, You're OK" or should it be "I'm not OK & Your Not OK", squeeze some 'Mars & Venus' juices and ignite it with some light energy therapy but Hold On!
A thunderous voice from one of the gods speaks and all is still. Here's what I want, throw in some CBT and GET. Booms the voice from the god, Wessely but Wait is it from Prism? Yes, good because I only want the best booms Wessely as he read the recipe from NICE.
Wessely stirs the pot. Wow did you see those vultures fly out of the pot. Don't worry about them, booms Wessely, that's what you call UNUM Vultures. They occasionally drop DSM manual shit everywhere. Search through the crap to find the latest psychobabble disorders so we can mix em in, he booms. Don't they need any scientific research for verification before they can come up with a disorder? Nope we just pull things out of the air and call it science and everyone believes the gods of psychobabble. We can make nothing into something and back into nothing.
Remember the good ole days when we use to label people with Parkinson, Diabetes, MS, Polio, SIDS as psychiatric disorders? Then the gods of science ruined it by linking them to organic conditions. What a field day we had playing around in medicine without having to actually examine an organ at treatment? Psychiatry? You Bet! Making nothing into something and back into nothing squawks Wessely. We can't measure Serotonin, Dopamine, Noradrenaline but we can sure give you medication but amount we don't know. We guesstimate. Is that science? To them it is. Heck, We don't take spect, pet, mri or fmri scans. It's really psychobabble between you and me...wink, wink. Yes and the medical profession must bow down to us the gods of psychobabble! Nothing into something and back into nothing, squawks Wessely.
