

adreno
PR activist
- Messages
- 4,841
I found the following study interesting. It describes how the balance of B3 and methyl groups ultimately determine health status and aging.
An illustration from the study:
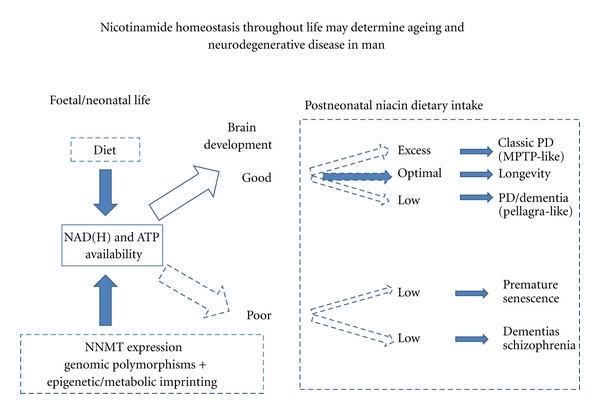
I must admit that I really don't have the knowledge to understand the implications of the article in depth. I'm hoping someone more knowledgeable than me will chime in.
But as I understand it, both under- or overdosing B3 and methyl groups will lead to serious health problems. The question is, how do we find the right balance? From the full text:
So what does this tell the many of us who are essentially megadosing on B vitamins and methyl donors? Is it safe at all? Or should we not supplement them? Are the problems related to ratio, dose or both? How would supplementing NAD or NADH change the picture?
If I seem confused, it's because I am.
Curr Gerontol Geriatr Res. 2012;2012:302875. Epub 2012 Mar 21.
Nicotinamide, NAD(P)(H), and Methyl-Group Homeostasis Evolved and Became a Determinant of Ageing Diseases: Hypotheses and Lessons from Pellagra.
Williams AC, Hill LJ, Ramsden DB.
Source
Neuropharmacology and Neurobiology, School of Clinical and Experimental Medicine, University of Birmingham, Edgbaston, Birmingham B15 2TT, UK.
Abstract
Compartmentalized redox faults are common to ageing diseases. Dietary constituents are catabolized to NAD(H) donating electrons producing proton-based bioenergy in coevolved, cross-species and cross-organ networks. Nicotinamide and NAD deficiency from poor diet or high expenditure causes pellagra, an ageing and dementing disorder with lost robustness to infection and stress. Nicotinamide and stress induce Nicotinamide-N-methyltransferase (NNMT) improving choline retention but consume methyl groups. High NNMT activity is linked to Parkinson's, cancers, and diseases of affluence. Optimising nicotinamide and choline/methyl group availability is important for brain development and increased during our evolution raising metabolic and methylome ceilings through dietary/metabolic symbiotic means but strict energy constraints remain and life-history tradeoffs are the rule. An optimal energy, NAD and methyl group supply, avoiding hypo and hyper-vitaminoses nicotinamide and choline, is important to healthy ageing and avoids utilising double-edged symbionts or uncontrolled autophagy or reversions to fermentation reactions in inflammatory and cancerous tissue that all redistribute NAD(P)(H), but incur high allostatic costs.
PMID:22536229
An illustration from the study:
I must admit that I really don't have the knowledge to understand the implications of the article in depth. I'm hoping someone more knowledgeable than me will chime in.
But as I understand it, both under- or overdosing B3 and methyl groups will lead to serious health problems. The question is, how do we find the right balance? From the full text:
Here we suggest the possibility that a hypervitaminosis B3 state, with both nicotinamide and N-methylnicotinamide having an optimal range, resulting from a western diet overrich in meat and vitamin supplements working alongside calorific excesses may be implicated in other modern disease phenomena. Meat eating is preferred where it is available, though during pregnancy it is a common dietary aversion, suggesting that it can be toxic in early development as does the presence of the detoxification enzyme, NNMT and evidence of acute toxicity with nicotinamide overdose and worries about red meat being a risk factor for some cancers [252–254]. Nicotinamide exposure can be high, in excess of five times the recommended daily amount (15mg/day) where diet has both cereals and “high energy” drinks supplemented with the vitamin and where there is an abundance of cheap meat and milk. This chronic overload can be envisioned as working through unbalancing NAD(H)-dependent systems, including SIRTs and PARPs or dehydrogenase pathways (for instance in cortisol metabolism), and through the direct effects of nicotinamide or N-methylated metabolites. NAD+ is the substrate for SIRTs and nicotinamide is an inhibitor, so dietary levels of NAD(H) precursors could act as both positive and negative influences on such systems. In the case of nicotinamide, dietary inputs are modulated in part by genetic determination of NNMT levels, with 24% of the population being high expressors. Nongenetic factors also modulate expression of the enzyme. These include nicotinamide itself, stress and the demands imposed on NAD(H) availability by growth, tissue repair and exercise. Interestingly, NNMT and other components of NAD(H) pathways are markedly induced in a variety of currently common cancers as well as in the metabolic syndrome, obesity, PD and autism [255–262].
So what does this tell the many of us who are essentially megadosing on B vitamins and methyl donors? Is it safe at all? Or should we not supplement them? Are the problems related to ratio, dose or both? How would supplementing NAD or NADH change the picture?
If I seem confused, it's because I am.