J Med Virol. 2017 Mar 17. doi: 10.1002/jmv.24810. [Epub ahead of print]
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Gulf War Illness patients exhibit increased humoral responses to the Herpesviruses-encoded dUTPase: Implications in disease pathophysiology.
Halpin P, Williams MV, Klimas NG, Fletcher MA, Barnes Z, Ariza ME.
Abstract
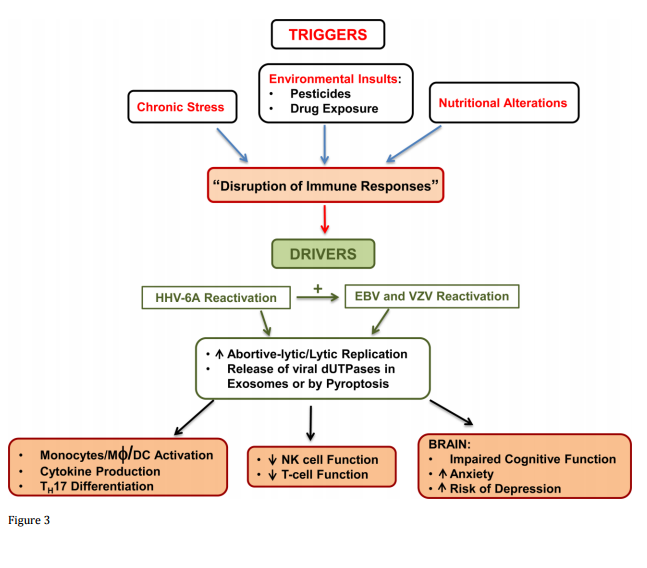
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Gulf War Illness (GWI) are debilitating diseases with overlapping symptomology and there are currently no validated tests for definitive diagnosis of either syndrome. While there is evidence supporting the premise that some herpesviruses may act as possible triggers of ME/CFS, the involvement of herpesviruses in the pathophysiology of GWI has not been studied in spite of a higher prevalence of ME/CFS in these patients. We have previously demonstrated that the deoxyuridine triphosphate nucleotidohydrolases (dUTPase) encoded by Epstein-Barr virus (EBV), human herpesvirus-6 (HHV-6), and varicella-zoster virus (VZV) possess novel functions in innate and adaptive immunity. The results of this study demonstrate that a significant percentage of patients with ME/CFS (30.91-52.7%) and GWI (29.34%) are simultaneously producing antibodies against multiple human herpesviruses-encoded dUTPases and/or the human dUTPase when compared to controls (17.21%). GWI patients exhibited significantly higher levels of antibodies to the HHV-6 and human dUTPases than controls (p = 0.0053 and p = 0.0036, respectively), while the ME/CFS cohort had higher anti-EBV-dUTPase antibodies than in both GWI patients (p = 0.0008) and controls (p < 0.0001) as well as significantly higher anti-human dUTPase antibodies than in controls (p = 0.0241). These results suggest that screening of patients' sera for the presence of various combinations of anti-dUTPase antibodies could be used as potential biomarkers to help identify/distinguish patients with these syndromes and better direct treatment. This article is protected by copyright. All rights reserved.
This article is protected by copyright. All rights reserved.
KEYWORDS:
Chronic Fatigue Syndrome; Epstein-Barr virus; Human herpesvirus 6; antibodies; deoxyuridine triphosphate nucleotidohydrolase; varicella-zoster virus
https://www.ncbi.nlm.nih.gov/pubmed/28303641
http://onlinelibrary.wiley.com/doi/10.1002/jmv.24810/abstract
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Gulf War Illness patients exhibit increased humoral responses to the Herpesviruses-encoded dUTPase: Implications in disease pathophysiology.
Halpin P, Williams MV, Klimas NG, Fletcher MA, Barnes Z, Ariza ME.
Abstract
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Gulf War Illness (GWI) are debilitating diseases with overlapping symptomology and there are currently no validated tests for definitive diagnosis of either syndrome. While there is evidence supporting the premise that some herpesviruses may act as possible triggers of ME/CFS, the involvement of herpesviruses in the pathophysiology of GWI has not been studied in spite of a higher prevalence of ME/CFS in these patients. We have previously demonstrated that the deoxyuridine triphosphate nucleotidohydrolases (dUTPase) encoded by Epstein-Barr virus (EBV), human herpesvirus-6 (HHV-6), and varicella-zoster virus (VZV) possess novel functions in innate and adaptive immunity. The results of this study demonstrate that a significant percentage of patients with ME/CFS (30.91-52.7%) and GWI (29.34%) are simultaneously producing antibodies against multiple human herpesviruses-encoded dUTPases and/or the human dUTPase when compared to controls (17.21%). GWI patients exhibited significantly higher levels of antibodies to the HHV-6 and human dUTPases than controls (p = 0.0053 and p = 0.0036, respectively), while the ME/CFS cohort had higher anti-EBV-dUTPase antibodies than in both GWI patients (p = 0.0008) and controls (p < 0.0001) as well as significantly higher anti-human dUTPase antibodies than in controls (p = 0.0241). These results suggest that screening of patients' sera for the presence of various combinations of anti-dUTPase antibodies could be used as potential biomarkers to help identify/distinguish patients with these syndromes and better direct treatment. This article is protected by copyright. All rights reserved.
This article is protected by copyright. All rights reserved.
KEYWORDS:
Chronic Fatigue Syndrome; Epstein-Barr virus; Human herpesvirus 6; antibodies; deoxyuridine triphosphate nucleotidohydrolase; varicella-zoster virus
https://www.ncbi.nlm.nih.gov/pubmed/28303641
http://onlinelibrary.wiley.com/doi/10.1002/jmv.24810/abstract