

katabasis
Senior Member
- Messages
- 159
Cannabigerol (CBG) is a minor phytocannabinoid found in cannabis. I have seen comparatively little discussion about it, despite its interesting pharmacological properties, which are somewhat distinct from the more commonly discussed phytocannabinoids such as THC, CBD, CBN, etc. The properties of CBG might be useful for some ME/CFS sufferers, and over the past few weeks I have seen a lot of benefits from using a high-CBG strain of cannabis.
Pharmacological Properties
Here is a good literature review on the pharmacology of CBG in general.
The properties of CBG overlap to an extent with those of cannabidiol (CBD). To begin with, it has low (micromolar) binding affinity at CB1 and CB2 receptors, though it seems researchers disagree about whether it acts as an antagonist or a weak partial agonist. In either case, this should allow CBG to mitigate the effects of CB1 agonists like THC, viz. reducing its psychoactive, recreational, and anxiogenic effects.
Additionally, CBG has comparable affinity to CBD and THC at various TRP channels – acting as an agonist at TRPA1, TRPV1, TRPV2, TRPV3, and TRPV4, and an antagonist at TRPM8. The topic of TRP channels is enormously complicated, but basically they are calcium channels that have various sensory functions, including sensing heat, touch, vibration, and pain, as well as modulating inflammation and immunity. It is believed that TRP channels are involved in the pain-relieving properties of cannabis. This paper has a good explanation of the role of TRP channels and how different cannabinoids affect them.
Finally, CBG is an agonist of PPAR-gamma receptors. Many phytocannabinoids activate this receptor, and some activate other PPAR receptors. PPAR receptors play a major role in metabolism, and are the target of several pharmaceutical drugs, such as PPAR-alpha agonists (fibrates) to treat dyslipidemia, and PPAR-gamma agonists (glitazones) to treat type 2 diabetes. This paper has a good explanation of the role of PPAR receptors and how different cannabinoids affect them.
CBG has some unique properties as well. Most notably it is a high affinity agonist of alpha-2 adrenergic receptors. These act as autoreceptors, so activating them reduces the release of norepinephrine/adrenaline, lowering blood pressure and heart rate. However, activation of these receptors also enhances cognition, especially executive function. You can see both of these effects in pharmaceutical alpha-2 agonists such as clonidine and guanfacine, which are primarily used to treat hypertension, but are often prescribed off-label to treat ADHD.
Additionally, CBG acts as a moderate affinity antagonist of 5-HT1A receptors. This is in contrast to CBD, which acts as a partial agonist at this receptor. Usually 5-HT1A agonism is seen as being more beneficial, producing antidepressant and anxiolytic effects. Nonetheless, I wonder whether there might be a role for 5-HT1A antagonism in ME/CFS, given the involvement of these receptors in the regulation of the HPA axis (see this paper). It seems that excessive ‘threat-specific release of 5-HT’ causes desensitization of 5-HT1A receptors, which then are no longer able to trigger downregulation of CRFR2 receptors. Perhaps antagonism of 5-HT1A receptors may cause them to upregulate, though this is merely speculation on my part.
Here is a paper which establishes how CBG affects alpha-2 adrenergic receptors and 5-HT1A receptors.
My Experience with CBG
Prior to developing ME/CFS, I was an occasional recreational user of cannabis. However, once this illness got me in its clutches, I became essentially intolerant of cannabis. Firstly, I became extraordinarily sensitive to it – even a tiny amount would provoke strong effects. These effects were also strangely inconsistent. Sometimes it would plunge me immediately into PEM, dramatically worsening my fatigue and flu-like pains, as well as causing nausea and even vomiting. Yet other times, it would not trigger PEM at all, even providing me with some minor pain relief, though I would usually experience a flu-like sort of ‘hangover’ after whatever small benefits it had given me had elapsed.
Cannabis contains a very wide variety of bioactive compounds, and I really wanted to identify which of these variables were responsible for the differing reactions I’d had. At first I experimented with taking CBD oil along with cannabis, though I never saw much of a difference from it. And then, for a while, I thought it had something to do with the terpenes present in cannabis, which are widely varied and all of which have unique properties.
But then, through sheer random luck, I bought a strain from my local dispensary (whimsically named ‘Slurricane’) that completely changed the type of experience I was getting from cannabis. The only distinguishing feature of this strain that I can identify is its high level of CBG - 0.26%, alongside 0.48% CBGA (most of which is likely converted to CBG during the smoking process). In fact, the only other measurable cannabinoids in Slurricane are THC and THCA themselves – no CBD, no CBN, etc.
As far as I can tell, many strains of cannabis have no CBG whatsoever, and those that do, have a much lesser amount (something like 0.05% combined would be typical). This may actually have something to do with the biology of the cannabis plant: CBGA is the biological precursor to THC and CBD, so high-CBG cannabis is, in some sense, ‘immature’. You can see why some cannabis growers would even see elevated CBG as wasted potential.
So what benefits has Slurricane given me? To begin with, it does not elevate my heart rate at all – something which can easily be attributed to CBG’s alpha-2 agonism. However, it does not lower my blood pressure, and sometimes even raises it. I am usually borderline hypotensive (90/60), and if I sit up or exert myself, my blood pressure will briefly normalize before eventually going back down to 90/60 or lower (my small fiber neuropathy is possibly the root cause of this issue, though after a year of IVIG I have seen little change to it, even as my nerve pain has improved considerably).
Slurricane also seems to have improved my tolerance to physical and mental exertion, improving from a 20 on the Bell CFIDS disability scale to something in the 30-40 range. It doesn’t have all that much effect on my baseline symptoms, but rather increases what I can do before I start risking PEM. This is a known benefit of cannabis for ME/CFS sufferers (it is on the list of ‘PEM busters’), so this may not be a direct benefit of CBG per se, though it remains to be seen why cannabis was having the opposite effect for me in the first place. One theory I have is that cannabis’s psychoactivity was a PEM trigger, viz. the rush of creative thoughts that were once a sought-after effect instead became part of an unavoidable mental overexertion.
On a similar topic, Slurricane is also unique in that it does not worsen my brain fog, though neither does it improve it. Of course, cannabis typically causes what amounts to brain fog in even healthy individuals, including impaired attention, short term memory, and coordination. Healthy friends of mine who have sampled this strain have also noted it to be especially clear-headed. Even at high doses, it has none of the overwhelming ‘brain folding in on itself’ feeling that cannabis sometimes causes. That CBG attenuates THC’s activity at CB1 receptors may contribute to this property, though I’ve never gotten this effect from CBD even though it should be able to do the same thing. I think the alpha-2 agonism may ultimately play a bigger role.
Without the risk of causing PEM or worsening brain fog, I have also been able to consume larger doses of cannabis. Aside from being convenient (since I no longer need to use a milligram scale to titrate my dose), this has also made the other typical benefits of cannabis far more accessible to me. Most significantly, Slurricane dramatically improves my IBS symptoms, including abdominal pain, cramping, nausea, and bloating. Some of my food intolerances have essentially vanished, which has been a great pleasure. Separately, cannabis improves my mood and facilitates creativity, though I suspect this benefit will dwindle after prolonged use.
Theories About CBG and Cannabis in ME/CFS
After identifying CBG as the likely factor, I wanted to test my theory further. It turns out that you can easily buy pure CBG online, so I was able to see how its effects held up in isolation. I found that CBG on its own has the same effects on heart rate and blood pressure, but does not seem to prevent PEM or any other ME/CFS symptoms. I think to a large degree CBG does not help ME/CFS per se, but rather it attenuates the negative effects of cannabis while retaining or enhancing its benefits. As proof of this concept, I combined a non-CBG-containing strain of cannabis (Animal Face x Banana Cream… how do they get these names?) with CBG isolate, and created a reasonable facsimile of Slurricane’s effects, if more sedating because of the presence of cannabinol (CBN) in the strain.
The fact that CBG can be used ad hoc like this is extremely convenient, as it may be difficult for other people to find a strain of cannabis which naturally contains high levels of CBG. If you want to buy CBG isolate and try this for yourself, keep in mind that the listed dosage may be higher than what is necessary – my dropper bottle of sublingual CBG isolate recommends a 50 mg dose, but I found even 5 mg to be more than sufficient (the ideal dose may be even lower than this, though I have yet to test it). The discrepancy makes sense to me – the effective CBG dosage in Slurricane, where it is less than 1% by weight, is probably less than a milligram for a ‘regular’ amount of cannabis. You can also compare this to the dosage of pharmaceutical alpha-2 agonists: 100 micrograms is typical for clonidine, and its potency is comparable if not lower than CBG itself.
While CBG alone did not produce such a large benefit for me, there may be some intrinsic benefit from alpha-2 agonism for some people with ME/CFS. The alpha-2 adrenergic receptor plays an important role in cardiovascular function, and may also play a minor role in pain processing, inflammation, and immune function.
One paper published recently showed that after exercise, ME/CFS sufferers (but not healthy controls) showed a marked difference in the expression of various genes, including for the alpha-2A subtype of adrenergic receptors.
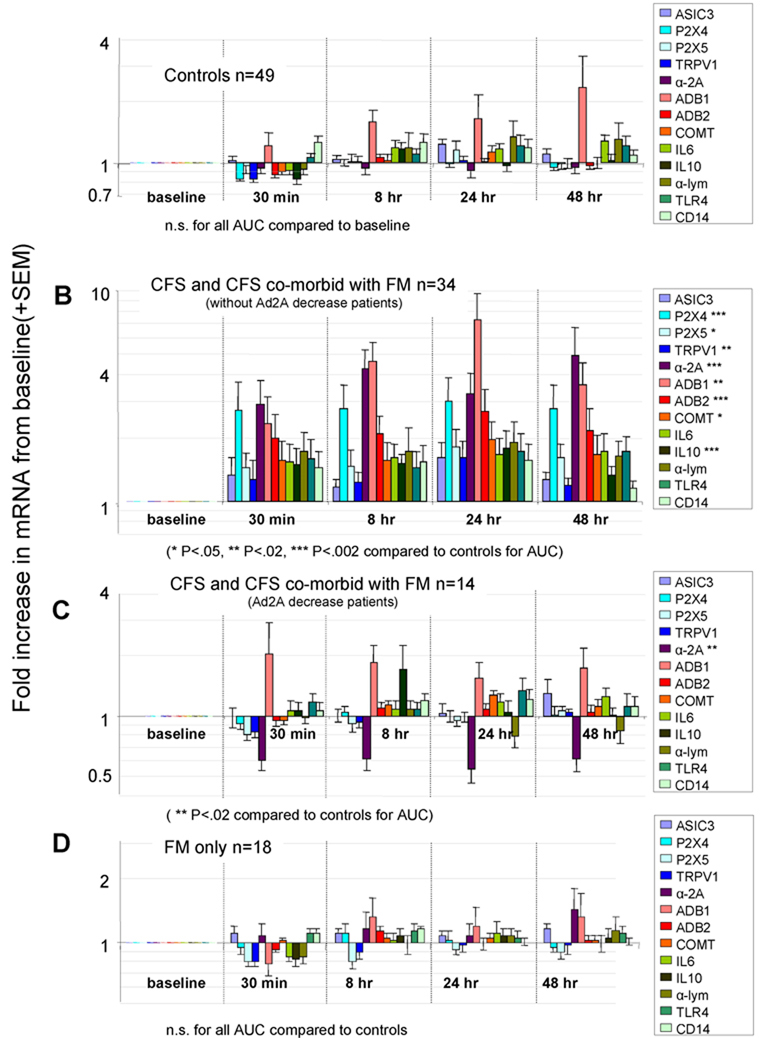
Unlike many of the other genes, the a2AR gene was significantly affected in patients with even mild-to-moderate symptoms. Note however that the effect was bimodal – patients could be separated into two groups: those that showed 3-4 fold increase of a2AR gene expression, and those that showed a roughly 40% decrease in a2AR gene expression. Perhaps only one of these groups will potentially benefit from alpha-2 adrenergic receptor agonism. It’s possible that those with hypofunction of this receptor benefit from increased activation of it, or in contrast, that activating the receptor causes it to downregulate in those where it is upregulated.
As it happens, there was also a recent study investigating whether the pharmaceutical alpha-2A agonist guanfacine is effective for ME/CFS when administered alongside NAC. The sample size is quite small, but there did seem to be some benefit. It remains to be seen whether these findings are broadly applicable; a previous study on another non-selective alpha-2 agonist, clonidine, found no benefit. Of course, clonidine is also an agonist of I1 imidazoline receptors, so that may be a confounding factor here.
It is also possible that the benefits I am seeing from Slurricane are due to some other factor not fully considered. It may be worth taking another look at those TRP channels I mentioned in the beginning of this post. Due to the variety in how phytocannabinoids activate these receptors, it is possible that CBG and THC combine to activate or block two or more of these receptors to produce an effect that neither can accomplish individually. And of course, cannabis products vary greatly in what terpenes are present, all of which have distinct pharmacological profiles, though my previous investigations of this topic were rather fruitless.
Conclusion
For the time being, I plan to continue using Slurricane regularly. I am a little worried about developing a physical dependence, but I recently stopped for a few days without having too much of a problem – merely a resurgence of my ‘normal’ ME/CFS symptoms, no worse than usual.
I want to know if anyone else has found CBG to be especially helpful. There was a surprising lack of results when I searched for it on these forums. It does seem to be a somewhat underappreciated phytocannabinoid even outside the ME/CFS community.
For those of you who get negative effects from cannabis, it may be worthwhile to experiment with high-CBG strains or even just CBG isolate added to low-CBG strains.
Pharmacological Properties
Here is a good literature review on the pharmacology of CBG in general.
The properties of CBG overlap to an extent with those of cannabidiol (CBD). To begin with, it has low (micromolar) binding affinity at CB1 and CB2 receptors, though it seems researchers disagree about whether it acts as an antagonist or a weak partial agonist. In either case, this should allow CBG to mitigate the effects of CB1 agonists like THC, viz. reducing its psychoactive, recreational, and anxiogenic effects.
Additionally, CBG has comparable affinity to CBD and THC at various TRP channels – acting as an agonist at TRPA1, TRPV1, TRPV2, TRPV3, and TRPV4, and an antagonist at TRPM8. The topic of TRP channels is enormously complicated, but basically they are calcium channels that have various sensory functions, including sensing heat, touch, vibration, and pain, as well as modulating inflammation and immunity. It is believed that TRP channels are involved in the pain-relieving properties of cannabis. This paper has a good explanation of the role of TRP channels and how different cannabinoids affect them.
Finally, CBG is an agonist of PPAR-gamma receptors. Many phytocannabinoids activate this receptor, and some activate other PPAR receptors. PPAR receptors play a major role in metabolism, and are the target of several pharmaceutical drugs, such as PPAR-alpha agonists (fibrates) to treat dyslipidemia, and PPAR-gamma agonists (glitazones) to treat type 2 diabetes. This paper has a good explanation of the role of PPAR receptors and how different cannabinoids affect them.
CBG has some unique properties as well. Most notably it is a high affinity agonist of alpha-2 adrenergic receptors. These act as autoreceptors, so activating them reduces the release of norepinephrine/adrenaline, lowering blood pressure and heart rate. However, activation of these receptors also enhances cognition, especially executive function. You can see both of these effects in pharmaceutical alpha-2 agonists such as clonidine and guanfacine, which are primarily used to treat hypertension, but are often prescribed off-label to treat ADHD.
Additionally, CBG acts as a moderate affinity antagonist of 5-HT1A receptors. This is in contrast to CBD, which acts as a partial agonist at this receptor. Usually 5-HT1A agonism is seen as being more beneficial, producing antidepressant and anxiolytic effects. Nonetheless, I wonder whether there might be a role for 5-HT1A antagonism in ME/CFS, given the involvement of these receptors in the regulation of the HPA axis (see this paper). It seems that excessive ‘threat-specific release of 5-HT’ causes desensitization of 5-HT1A receptors, which then are no longer able to trigger downregulation of CRFR2 receptors. Perhaps antagonism of 5-HT1A receptors may cause them to upregulate, though this is merely speculation on my part.
Here is a paper which establishes how CBG affects alpha-2 adrenergic receptors and 5-HT1A receptors.
My Experience with CBG
Prior to developing ME/CFS, I was an occasional recreational user of cannabis. However, once this illness got me in its clutches, I became essentially intolerant of cannabis. Firstly, I became extraordinarily sensitive to it – even a tiny amount would provoke strong effects. These effects were also strangely inconsistent. Sometimes it would plunge me immediately into PEM, dramatically worsening my fatigue and flu-like pains, as well as causing nausea and even vomiting. Yet other times, it would not trigger PEM at all, even providing me with some minor pain relief, though I would usually experience a flu-like sort of ‘hangover’ after whatever small benefits it had given me had elapsed.
Cannabis contains a very wide variety of bioactive compounds, and I really wanted to identify which of these variables were responsible for the differing reactions I’d had. At first I experimented with taking CBD oil along with cannabis, though I never saw much of a difference from it. And then, for a while, I thought it had something to do with the terpenes present in cannabis, which are widely varied and all of which have unique properties.
But then, through sheer random luck, I bought a strain from my local dispensary (whimsically named ‘Slurricane’) that completely changed the type of experience I was getting from cannabis. The only distinguishing feature of this strain that I can identify is its high level of CBG - 0.26%, alongside 0.48% CBGA (most of which is likely converted to CBG during the smoking process). In fact, the only other measurable cannabinoids in Slurricane are THC and THCA themselves – no CBD, no CBN, etc.
As far as I can tell, many strains of cannabis have no CBG whatsoever, and those that do, have a much lesser amount (something like 0.05% combined would be typical). This may actually have something to do with the biology of the cannabis plant: CBGA is the biological precursor to THC and CBD, so high-CBG cannabis is, in some sense, ‘immature’. You can see why some cannabis growers would even see elevated CBG as wasted potential.
So what benefits has Slurricane given me? To begin with, it does not elevate my heart rate at all – something which can easily be attributed to CBG’s alpha-2 agonism. However, it does not lower my blood pressure, and sometimes even raises it. I am usually borderline hypotensive (90/60), and if I sit up or exert myself, my blood pressure will briefly normalize before eventually going back down to 90/60 or lower (my small fiber neuropathy is possibly the root cause of this issue, though after a year of IVIG I have seen little change to it, even as my nerve pain has improved considerably).
Slurricane also seems to have improved my tolerance to physical and mental exertion, improving from a 20 on the Bell CFIDS disability scale to something in the 30-40 range. It doesn’t have all that much effect on my baseline symptoms, but rather increases what I can do before I start risking PEM. This is a known benefit of cannabis for ME/CFS sufferers (it is on the list of ‘PEM busters’), so this may not be a direct benefit of CBG per se, though it remains to be seen why cannabis was having the opposite effect for me in the first place. One theory I have is that cannabis’s psychoactivity was a PEM trigger, viz. the rush of creative thoughts that were once a sought-after effect instead became part of an unavoidable mental overexertion.
On a similar topic, Slurricane is also unique in that it does not worsen my brain fog, though neither does it improve it. Of course, cannabis typically causes what amounts to brain fog in even healthy individuals, including impaired attention, short term memory, and coordination. Healthy friends of mine who have sampled this strain have also noted it to be especially clear-headed. Even at high doses, it has none of the overwhelming ‘brain folding in on itself’ feeling that cannabis sometimes causes. That CBG attenuates THC’s activity at CB1 receptors may contribute to this property, though I’ve never gotten this effect from CBD even though it should be able to do the same thing. I think the alpha-2 agonism may ultimately play a bigger role.
Without the risk of causing PEM or worsening brain fog, I have also been able to consume larger doses of cannabis. Aside from being convenient (since I no longer need to use a milligram scale to titrate my dose), this has also made the other typical benefits of cannabis far more accessible to me. Most significantly, Slurricane dramatically improves my IBS symptoms, including abdominal pain, cramping, nausea, and bloating. Some of my food intolerances have essentially vanished, which has been a great pleasure. Separately, cannabis improves my mood and facilitates creativity, though I suspect this benefit will dwindle after prolonged use.
Theories About CBG and Cannabis in ME/CFS
After identifying CBG as the likely factor, I wanted to test my theory further. It turns out that you can easily buy pure CBG online, so I was able to see how its effects held up in isolation. I found that CBG on its own has the same effects on heart rate and blood pressure, but does not seem to prevent PEM or any other ME/CFS symptoms. I think to a large degree CBG does not help ME/CFS per se, but rather it attenuates the negative effects of cannabis while retaining or enhancing its benefits. As proof of this concept, I combined a non-CBG-containing strain of cannabis (Animal Face x Banana Cream… how do they get these names?) with CBG isolate, and created a reasonable facsimile of Slurricane’s effects, if more sedating because of the presence of cannabinol (CBN) in the strain.
The fact that CBG can be used ad hoc like this is extremely convenient, as it may be difficult for other people to find a strain of cannabis which naturally contains high levels of CBG. If you want to buy CBG isolate and try this for yourself, keep in mind that the listed dosage may be higher than what is necessary – my dropper bottle of sublingual CBG isolate recommends a 50 mg dose, but I found even 5 mg to be more than sufficient (the ideal dose may be even lower than this, though I have yet to test it). The discrepancy makes sense to me – the effective CBG dosage in Slurricane, where it is less than 1% by weight, is probably less than a milligram for a ‘regular’ amount of cannabis. You can also compare this to the dosage of pharmaceutical alpha-2 agonists: 100 micrograms is typical for clonidine, and its potency is comparable if not lower than CBG itself.
While CBG alone did not produce such a large benefit for me, there may be some intrinsic benefit from alpha-2 agonism for some people with ME/CFS. The alpha-2 adrenergic receptor plays an important role in cardiovascular function, and may also play a minor role in pain processing, inflammation, and immune function.
One paper published recently showed that after exercise, ME/CFS sufferers (but not healthy controls) showed a marked difference in the expression of various genes, including for the alpha-2A subtype of adrenergic receptors.
Unlike many of the other genes, the a2AR gene was significantly affected in patients with even mild-to-moderate symptoms. Note however that the effect was bimodal – patients could be separated into two groups: those that showed 3-4 fold increase of a2AR gene expression, and those that showed a roughly 40% decrease in a2AR gene expression. Perhaps only one of these groups will potentially benefit from alpha-2 adrenergic receptor agonism. It’s possible that those with hypofunction of this receptor benefit from increased activation of it, or in contrast, that activating the receptor causes it to downregulate in those where it is upregulated.
As it happens, there was also a recent study investigating whether the pharmaceutical alpha-2A agonist guanfacine is effective for ME/CFS when administered alongside NAC. The sample size is quite small, but there did seem to be some benefit. It remains to be seen whether these findings are broadly applicable; a previous study on another non-selective alpha-2 agonist, clonidine, found no benefit. Of course, clonidine is also an agonist of I1 imidazoline receptors, so that may be a confounding factor here.
It is also possible that the benefits I am seeing from Slurricane are due to some other factor not fully considered. It may be worth taking another look at those TRP channels I mentioned in the beginning of this post. Due to the variety in how phytocannabinoids activate these receptors, it is possible that CBG and THC combine to activate or block two or more of these receptors to produce an effect that neither can accomplish individually. And of course, cannabis products vary greatly in what terpenes are present, all of which have distinct pharmacological profiles, though my previous investigations of this topic were rather fruitless.
Conclusion
For the time being, I plan to continue using Slurricane regularly. I am a little worried about developing a physical dependence, but I recently stopped for a few days without having too much of a problem – merely a resurgence of my ‘normal’ ME/CFS symptoms, no worse than usual.
I want to know if anyone else has found CBG to be especially helpful. There was a surprising lack of results when I searched for it on these forums. It does seem to be a somewhat underappreciated phytocannabinoid even outside the ME/CFS community.
For those of you who get negative effects from cannabis, it may be worthwhile to experiment with high-CBG strains or even just CBG isolate added to low-CBG strains.