There are some in the ME/CFS medical field that believe ME/CFS is 'MS Light' or 'Atypical MS'. The reason I post these articles is the fact that research in one area may spill over into another area of research or the fact that researchers reviewing a site may look at the research in another disease category that could be related to theirs and it might raise their interest level.
Futhermore, research may be further ahead in another field that ME/CFS researchers wish to explore if they had the funding and the researchers to explore such as EBV, HERVs, Autoimmune diseases, Fibromyalgia, Lyme etc.
Permission to post
Prof. Permission to repost by Prof. G
NOTE: Paradigm Shift in MS Research
MS Was Considered T-Cell Mediated Autoimmune Disease
https://multiple-sclerosis-research.../ms-is-b-cell-disease-and-memory-b-cells.html
MS is a B cell Disease and Memory B cells are the Target for therapy
Baker D, Marta M, Pryce G, Giovannoni G, Schmierer KMemory B cells are major targets for effective immunotherapy in relapsing multiple sclerosis. EBioMedicine 2017
(CLICK FOR FULL STORY).
http://www.ebiomedicine.com/article/S2352-3964(17)30045-2/pdf
Although multiple sclerosis (MS) is considered to be a CD4,Th17-mediated autoimmune disease, supportive evidence is perhaps circumstantial, often based on animal studies, and is questioned by the perceived failure of CD4-depleting antibodies to control relapsing MS. Therefore it was of interest to find that current MS-treatments, believed to act via T cell inhibition including: beta-interferons, glatiramer acetate, cytostatic agents, dimethyl fumarate, fingolimod, cladribine, daclizumab, rituximab/ ocrelizumab physically, or functionally in the case of natalizumab, also depleted CD19+,CD27+ memory B cells. This depletion was substantial and long-term following CD52 and CD20-depletion, and both also induced long-term inhibition of MS with few treatment cycles, indicating induction-therapy activity. Importantly, memory B cells were augmented by B cell activating factor (atacicept) and tumor necrosis factor (infliximab) blockade that are known to worsen MS. This creates a unifying concept centered on memory B cells that is consistent with therapeutic, histopathological and etiological aspects of MS.
Following on from our recent post (major target for treatment), it is clear that some of you don't want to read the full story (if you do click here) and would like it summarized
http://www.ebiomedicine.com/article/S2352-3964(17)30045-2/pdf
Highlights
Memory B cells express CD19+, CD27+ and CD21, CD20, CD25, CD49d, CD52, S1P1, and have higher endogenous proliferative background than T cells.
Memory B cells express CD21, which is the EBV receptor
Memory B cells are elevated in MS and accumulate in the CNS in MS
Memory B cells are depleted or functionally silenced by all treatments of MS.
Memory B cell depletion potential correlates with drug efficacy
Memory B cell augmentation is associated with MS worsening
Memory B cell-tailored therapy may allow personalised and safer induction treatment
ProfG was set to go to Lisbon to present at an antibody engineering meeting to talk on "How do antibodies work in MS". Rather than try present his 65 slides in 30min, we aimed to see if we could answer the question.
So do alemtuzumab, rituximab/ocrelizumab, daclizumab and natalizumab have anything in common?
Although alemtuzumab depletes T cells, it was evident that memory B cell depletion is marked and it set us thinking as an alternative to the T cell hypothesis.
Surprisingly all agents that inhibit MS could cause depletion of memory B cells. Interestingly those that worsen MS cause elevated memory B cell responses in some people.
Surprise surprise, we found papers where some people had similar thoughts (there is no such things as an original idea) but in most cases this was a throw-away idea and was dumped in the midst of many other concepts. However, we had more meat on the story by that time, we saw others work.
One of the odd one being (F below) natalizumab that augmented numbers in the blood, but as the idea is that it stops trafficking into the brain, this should be expected.
Daclizumab is another one of the odd treatments. However once you realise that memory B cells express CD25 and you can see that dacliziumab depletes CD19 B cells, you get in a groove and start looking for it, and find supportive evidence pop-up all over the place. There is also a poster on teriflunomide which supports this concept too.
Some publishers wanted too much money for us to include every example for every treatment in the publication. But we give some references if you want to look and the paper is "open source".
So this was revelation part one. The next one has additional implications.
Importantly the B memory cell idea gives more insight on ocrelizumab to suggest that CD20 treatment may be over-used to achieve benefit.
The data can be interpreted to suggest that ocrelizumab and alemtuzumab could work in the same way (bad news for both companies, sorry).
They are probably "both" induction therapies of PIRT (pulsed immune reconsitution therapies)
One wonders why such important data has not been properly published? It was dumped in an ECTRIMS abstract in 2012 and an AAN abstract in 2013 (where we found them. Do neurologists have enough time in a couple of hours to see and digest a 1000 posters?) and so there is no excuse from the companies or authors that they have not had enough time to publish the work. There are enough journals desperate for papers.
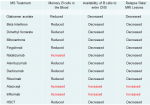
Now look at the figure above and you will see there is a clear inference that memory B cell levels may be a biomarker for treatment responsiveness.
Looking at figure E it shows only a few people on beta interferon have less than 20% of memory CD19 B cells. Are these the responders? Fingolimod (E) has more, but some failures. In (B) there is more depletion with mitoxantrone and (C) rituximab shows a lot of depletion, which is consistent with its high efficacy in MS.
There are studies in other conditions that use rituximab showing that CD19, CD27 numbers rise in the 4 months before a relapse and can be used as a biomarker to inform on retreatment such that one may be able to use 2/3 less rituximab, which is both safer and cheaper and takes us some way forward to personalised medicine.
In some treatments there are some indivudals that make more memory B cells and treatments that do this have in some cases been associated with MS worsening
Importantly memory B cells are the population of cells that accumulates in the CNS in MS and they express the EBV receptor, so depletion of the memory B cell subset depletes the antigen presenting cell that can activate T cells, or perhaps it eliminates the viral reservoir and removes the trigger of MS.
In many cases both unswitched (Have not change the antibody subtype they can produce) and switched (IgM and IgD are down regulated and IgG is upregulated from the unswtichted to switched) memory B cells are affected. Which subset is the critical one, the one that has already been reported to be increased in MS.
The T cell immunologists, will have a hard time with this concept, and their stock answer it is because it blocks antigen presentation, but the simple answer is what data argues against this concept?
Is the data that suggests a T cell action solid or is it simply circumstantial. Have a read of the paper for your self it is open access (CLICK to DOWNLOAD).
We suggests ways forward to perhaps make treatments safer and better.
Maybe the data miners out there can do some trawling and see what's against the idea. Send them (paper titles) in and lets see if the idea flies.
We have thrown down the gauntlet, and if read, people will either agree or disagree.
Reactions:
Posted by MouseDoctor at 07:00
Email ThisBlogThis!Share to TwitterShare to FacebookShare to Pinterest
20 comments:
Iain OFriday, February 03, 2017 7:11:00 am
I believe in the B cell hypothesis you are offering here, but I think that there is something else at play that is still elusive. If you are selective in what you look for in terms of treatment impact, I wonder if you would find other changes in the body occurring with medical intervention for MS? Perhaps you would show that there are other depletions... and that would send you down a totally different rabbit hole.
Clearly B cells are an issue. But are they the whole issue?
And if you do identify rogue B cells as the culprit - then what does that mean, not just for prevention, but for the root cause of the disease? What are the correlations between B cells and Vitamin D? B cells and EBV?
Once upon a time T cells were seen, again and again, as the target cell. Research went out to support that dogma, and did so again and again. Beware the mistakes of the past.
Replies
MouseDoctorFriday, February 03, 2017 9:29:00 am
Following dogma is a problem as it does become self sustaining
So must get next paper written to question that EAE experiments are the way to go. Another lead balloon coming your way....Yes we should save the science lemmings and save a load of beasties in the process.
MouseDoctorFriday, February 03, 2017 9:20:00 am
Please read the final paragraph of the paper. The relationship between B cell memory and EBV is there. These cells are the B cells infected by EBV. I suspect vitamin D is important in repertoire and immune development. There is a clear link with diabetes and vitamin D and remember that diabetes starts in childhood so the inference is that the impact will be early in life hence the month of birth effects.
It seems to be a week for rabbit holes and so you are right about putting all eggs in one basket.Quite dangerous but for a long long time most of those eggs have been T cell eggs.
There is a problem that this phenotyping is done using flow cytometry and this outputs in proportions so as one goes down something else goes up. Is it B reg?
But there are some testable questions we are waiting for pharma to trawl their trial data
Replies
AnonymousFriday, February 03, 2017 10:16:00 am
hahaha... while (i thought) your efforts to link b cells to ebv were a tiny bit less convincing (in the context of causation) then your table setting out the control/destruction of memory b cells by current dmts thought to control ms on basis of t cell action, i was so very impressed by your dedication to tie it all together with a convincing theory
")
you made such a compelling argument: and i agree - disagree with it by using evidence against the info in table 4: if you can do that, we will be all ears to hear the arguments because they could be informative.
but if you can't do that.. are you just arguing a religion?
MouseDoctorFriday, February 03, 2017 10:27:00 am
Causation and EBV is a profG thang and there have been numerous reviews on this. I need to do more reading on this.
OK wait till Monday and I,ll use the same logic to tie memory T cells into the table 4. How,s that?
MouseDoctorFriday, February 03, 2017 10:32:00 am
As to evidence against I can't remember seeing much using the searches done, maybe we can pick populations and do it all again.
MouseDoctorFriday, February 03, 2017 10:37:00 am
CD21 is the receptor EBV uses to infect cells. This is a B cell receptor that binds inactivated C3 complement C3d
CinaraSaturday, February 04, 2017 6:59:00 am
I'm not going to give personal or anecdotal reports, but months before my first relapse in my life I had a relapse of a mononucleosis that I thought would kill me.
If EBV is linked even to cancers, why would not it be associated with other diseases?
Until the scientific community and society itself, it's thought that the outbreak of Zika Virus was directly linked to the numerous cases of Microcephaly in infants in Brazil, there was a last flurry of disbelief and denial.
AnonymousSaturday, February 04, 2017 12:13:00 pm
If EBV is linked even to cancers, why would not it be associated with other diseases?
I suspect (but could be wrong) that there could be a number of diseases thought to be linked to EBV (but not listed in the 'official' list of EBV disease associations). EBV Zika et al..... why on earth would our world pollies care about them while there is no direct association? zika turned out to be visible and so some money was spent on it (on research and on other measures)... but if you can't see it, why care about it? most ebv related diseases don't come with pictures of babies with abnormally shaped heads...
CinaraSaturday, February 04, 2017 8:30:00 pm
You may even be right that many of the EBV/related diseases "don't cause deformations", but what if EBV really is the driving force behind the development of MS in genetically susceptible individuals?
If you have MS you may not have an "apparent" strain on your head because of a virus, but you are having your CNS eaten "inside."
So your statement is somewhat incoherent.
CinaraSaturday, February 04, 2017 8:46:00 pm
Every hypothesis has its "Achilles heel." For example the gender gap the development of MS. Women further develop the disease, it's not an inherited disease but has common genetic factors involved. But someone asks, "How do you explain the cases of MS in men? Is it really related because GA plus oestradiol did not stop the disease?" And a lot of whys who could put hypotheses to the ground. But the important question is: why Ocrelizumab can act on Primary Progressive MS, and the other DMTs have not been able to do this? It is already clear that there is something with B lymphocytes.
So checking if EBV can be behind this is perfectly plausible, since it infects B cells.
If it were so nobody would but try to find out the cause and involved factors of anything, illness some.
MouseDoctorSaturday, February 04, 2017 10:13:00 pm
why ocrelizumab works in progressive MS. I suspet that because it was loaded with young pwMs with active disease that would respond to peripherally acting immunosuppressive agents
MouseDoctorFriday, February 03, 2017 9:34:00 am
The funny thing about this journal as it asks for the outstanding questions so our ideas for free again...Happy experimenting
Replies
AnonymousFriday, February 03, 2017 10:04:00 am
I know what you mean about ideas for free MD. I was doing my postgrad and my supervisor said they hadn't heard before of one idea I suggested. Fast forward a year and I look on their university website page and it said that they are currently working with that idea!
I know try and keep my research ideas quiet which is hard to do when I'm enthusiastic.
Reply
AnonymousFriday, February 03, 2017 11:28:00 am
This looks to me like a good explanation for the natalizumab withdrawal rebound effect. Natalizumab increases b-cells in the blood but blocks them from entering the CNS.
When one goes off natalizumab the increased number of b-cells in the blood are now free to enter CNS and lead to the dreaded rebound effect.
Reply
Scottish CliveFriday, February 03, 2017 4:13:00 pm
How long do you think it will be before Pharma accepts this and focus primarily on B-cells? What does this means for drugs in the pipeline such as ublituximab? Or do you think we need to start from scratch again in developing an effective, targeted treatment?
Replies
MouseDoctorFriday, February 03, 2017 4:51:00 pm
Pharma are already focusing on B cells, but they have not always got it right like atacicept and tabalumab, but there are other ways to target these cells.
Ublituximab is another CD20 antibody, like ocrelizumab and ofatumumab they will need to do their trials just like Roche and Novartis have done.
However you can start from scratch to make more focused treatments
Reply
Daniel BakerFriday, February 03, 2017 10:18:00 pm
Interesting.....
http://www.abc.net.au/news/2017-02-...-identify-types-of-multiple-sclerosis/8236336
Replies
AnonymousSaturday, February 04, 2017 1:13:00 am
the actual article published -
http://www.nature.com/articles/srep41473
MouseDoctorSaturday, February 04, 2017 4:44:00 am
thansk will have a look
Reply