I'm actually looking at these
TRP channels which were reported as being upregulated in this study. They specifically let mainly calcium inside, but also can let in other ions.
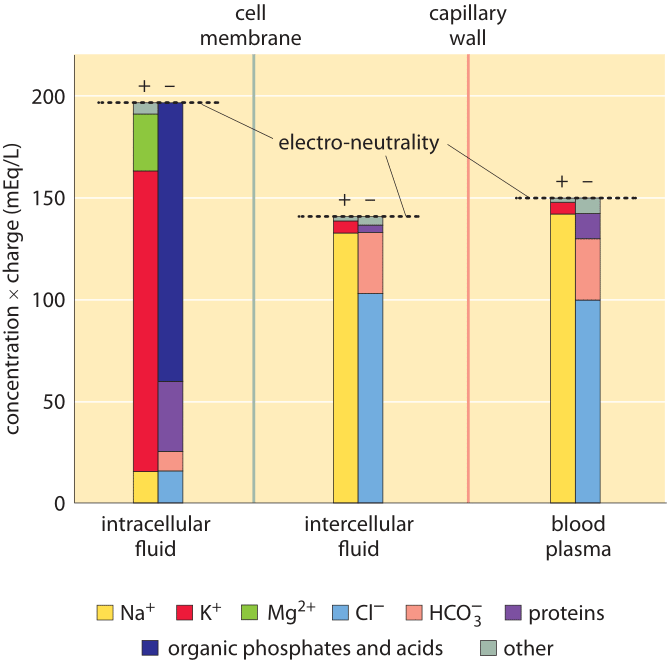
Calcium is a very interesting ion. The thing about calcium, is that there is regularly almost no calcium inside a cell:
The intracellular calcium level is kept relatively low with respect to the extracellular fluid, by an approximate magnitude of 12,000-fold. (
https://en.wikipedia.org/wiki/Calcium_in_biology#Vertebrates)
Calcium is used as a secondary messenger in cells. It is used in things that require
sensitivity. There is almost no calcium in cells, and the gradient is so steep, because the cells need radio
silence. Touch, heat, pain are all integral to our survival, and need to be very sensitive. Almost no calcium in cells = no noise.
The low amount of calcium in cells is how your touch is so sensitive that you can feel stuff like a hair in your fingertips. If it was K or NA ions that regulated touch, there is already so many ions moving about, that it would create a ton of noise.
Calcium has such a steep gradient, that is requires one ATP for every calcium ion extricated using
plasma membrane Ca2+ ATPase. Also on that page, you can see that even with a whole ATP, this process goes
slowly. The ion really wants to flow back into the cell.
By the nature of sensitivity, ions need to both flow into a cell very fast, and there needs to be very little of the ions in a cell. This means that the gradient is super steep, and this gradient is super hard to climb. It is like forcing these calcium cells to climb up a steep mountain in order to get out.
Na+/K+-ATPase on the other hand, the transporter that uses 1/5th of a cell's energy, uses
one ATP to move
three Na ions and
two K ions, BOTH against their ion gradient.
You can see how energy consuming excess calcium is... all because the ion gradient is a cliff.
If calcium needs to be extricated quickly, then it needs to
recruit the potential energy of the ion gradient of Na, using the sodium-calcium exchanger (NCX) in order to push it out much faster.
My theory is that phenibut helps me because it keeps both the NA and ATP higher, where normally they would be used up by pumping out calcium. This means that cells operate better because they have enough NA to sustain normal function. And ATP doesn't run out either. * Turns out the NCX actually brings Na in, going from a higher concentration to a lower concentration.
My theory is that phenibut helps me because it keeps Na lower and ATP higher, where normally they would be used up by pumping out calcium. This means that cells operate better because they have enough NA to sustain normal function. And ATP doesn't run out either.
It is also becoming extremely clear why Fibromyalgia and CFS are so closely linked.
Maybe this is also why I can last almost exactly 1 hour until I run out of energy after waking up, because my cellular NA stores run out, and I'm forced to swap over from
NCX to
plasma membrane Ca2+ ATPase. Before 1 hour passes, I'm an extremely high functioning individual and most of my CFS symptoms aren't there. Afterwards, suddenly I'm using up a huge amount of ATP, and
my NA stores are depleted Na concentration is way too high, fucking up TONS of functions in my cells.
It is like a switch, I go from super intelligent thought and suddenly just stop 1 hour in. It's like if you were talking and had a stroke, you just stop mid way, it happens instantly. I can watch my thoughts as I turn borderline retard.
EDIT: One last note, is that the
TRP channels implicated in the study, are
channels and not
transporters. In channels, when they open, it is like sliding down a slide. With transporters, on the other hand, it is
much slower. If something goes wrong with these channels, things can go
really wrong.
Cavity in a carrier protein is not open simultaneously to the both environment (extracellular and intracellular). Either its inner gate is open, or outer gate is open, Carrier has binding sites, but porins and channel proteins have not. When a channel is opened,
thousands to millions of ions can pass through the membrane in one time, but only one or a small amount of molecules can pass through a carrier molecule.(
source)
Goodnight everyone I'l be back tomorrow with more ion channel facts. (and also more proofreading here)