Murph
:)
- Messages
- 1,799
When it comes to effort preference the findings seems to hinge on this one test about whether you'd choose to press a button with the little finger of your non-dominant hand 98 times in 21 seconds or prefer to do 30 button presses with your usual index finger, for seven seconds, in return for various small prizes (the hard task prizes are bigger).
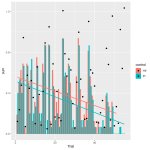
The relevant outcome is not how you do at the test - but which test you choose.

Here's how patients and controls did (this chart is in the supplementary material). At the beginning, about 45% of patients chose the hard task, compared to about 55% of controls. (presumably this is 8 of 17 patients and 12 of the 21 controls?). It went down from there (the data in this chart is smoothed not raw). The decay rates were similar between groups. By about trial 15 patients were as likely to choose the hard task as patients had been at the start.
The p-value for between group difference was p=.04.

It's a funny sort of a test, invented in 2009 to measure anhedonia in the depressed. It is regularly cited, so I guess it's part of the accepted literature on effort. An important question to ask is whether it has been validated for use in a group with a fatiguing illness, or whether that might confound the conclusions drawn from it.
Another question might be whether it was controlled for biological sex; the total control group had ever so slightly more men in it and the original 2009 paper finds men more likely to choose the hard task.
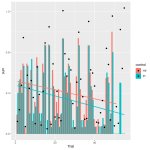
The relevant outcome is not how you do at the test - but which test you choose.
Here's how patients and controls did (this chart is in the supplementary material). At the beginning, about 45% of patients chose the hard task, compared to about 55% of controls. (presumably this is 8 of 17 patients and 12 of the 21 controls?). It went down from there (the data in this chart is smoothed not raw). The decay rates were similar between groups. By about trial 15 patients were as likely to choose the hard task as patients had been at the start.
The p-value for between group difference was p=.04.
It's a funny sort of a test, invented in 2009 to measure anhedonia in the depressed. It is regularly cited, so I guess it's part of the accepted literature on effort. An important question to ask is whether it has been validated for use in a group with a fatiguing illness, or whether that might confound the conclusions drawn from it.
Another question might be whether it was controlled for biological sex; the total control group had ever so slightly more men in it and the original 2009 paper finds men more likely to choose the hard task.
Last edited: