I think there should be some focus on the table in the Appendix that actually looked at the effects of CBT and GET after treatment so thought I would give it it's own thread:
View attachment 13280
The authors suggest that it is the CBT and GET after APT and specialist medical care alone that is the reason the differences between the groups disappeared. However the table doesn't bear this out.
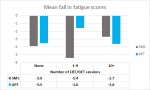
Indeed those that had 10 or more sessions of CBT and GET tended to have the lowest improvements of the three groups ((i)10+ sessions of CBT and GET post-trial; (ii) 1-9 sessions of CBT or GET and (iii) no sessions of CBT or GET post trial). (We're looking at the first two columns)
(For the Chalder Fatigue Questionnaire (CFQ), the lower the score the better the result. For the SF-36 physical functioning subscale, it's the opposite: the higher the score the better. The main thing of interest is the change scores i.e. mean difference).
Thanks for posting this table. Struggling a bit to understand it - have a couple of questions. First this quote
Dr Kimberley Goldsmith from the Institute of Psychiatry, Psychology & Neuroscience at King’s College London said: We found that participants who had originally been given SMC or APT appeared to be doing as well as those who had CBT or GET in the longer term. However as many had received CBT or GET after the trial, it does not tell us that these treatments have as good a long term outcome as CBT and GET.’
Am I right in thinking that the second sentence is actually inaccurate as they have measured the outcomes of those in the SMC and APT group who then went on to have CBT / GET? (the top two and the middle two rows of the table) compared to those who haven't. And the improvements were worse for the +10 sessions of CBT / GET.
Sorry if this is a daft question but is the mean difference the average (i.e. all added up and divided by the number of participants as opposed to say median) difference of the participants SF36 and CFQ scores at the end of the trial and then at the end of the 52 week review?
And the researchers are saying that there was more improvement in the CBT / GET groups than SMC and APT by the end of the trial, but at the end of the 30 months this improvement had gone, and this is because the SMC and APT groups went on to have sessions of CBT / GET? You are saying that those who had 10+ sessions of CBT / GET (deemed by the researchers as adequate treatment) actually had lower improvement levels than 1-9 of CBT / GET or no CBT / GET. The 1-9 sessions improvement level is a bit confusing though as it is higher (if I have read the tables correctly) than that for 10+ sessions and no sessions.
I'm struggling with interpreting the mean difference scores in the context that you mention. In the second row of the table (SF36+10 or sessions of CBT / GET) the mean differences are
APT 5.4
SMC 5.2
CBT 14.3
GET 2.8
Does that mean that in this group (+ 10 sessions CBT / GET) the most improvement was in the CBT arm , and the least in the GET arm with APT and SMC in the middle?
And for the CFQ + 10 sessions CBT / GET the most improvement was CBT (-6.4), then APT, then GET, then SMC? Or have I got it the wrong way round?
Then looking down the table, for the SMC and APT group the mean differences for SF36 and CFQ were
+ 10 sessions of CBT / GET: 5.4 and 5.2 (CFQ -2.7 & -3.6)
1 - 9 sessions of CBT / GET: 11.6 and 11.3 (CFQ -5.4 & -1.6)
No post trial CBT / GET: 5.8 and 8.5 (CFQ -3.9 & -3.5)
Does this mean that the most improvement was in the 1-9 sessions of CBT / GET on the SF36 scale and on the CFQ this group had the most improvement -5.4 for SMC?
Thanks but no worries if you don't want to plough through all those questions