SDSue
Southeast
- Messages
- 1,066
If I could leave my home, I'd hand-deliver a copy of the report to the Mayo Clinic.


Literature Search
•Post-exertional malaise
•Orthostatic intolerance and autonomic dysfunction
•Neurocognitive manifestations
•Sleep-related symptoms
•Symptom Constructs and Clusters
•Immune impairment
•Neuroendocrine manifestations
•Fatigue
•Pain
•Infection
The committee reviewed literature on a number of symptoms in ME/CFS patients:
Targeted literature searches are in bold.
Chronic Fatigue Syndrome gets yet another name
What's in a name? Chronic Fatigue Syndrome, a condition that debilitates as many as 2.5 million people in the US with exhaustion, should be renamed Systemic Exertion Intolerance Disease, according to the US Institute of Medicine (IOM).
- 17:33 10 February 2015 by Andy Coghlan
- Magazine issue 3008. Subscribe and save
As well as the name-change, the IOM has this week proposed a five-point checklist for diagnosis. Because the cause of the condition, also known as myalgic encephalomyelitis or ME, remains unknown, identifying the condition can be difficult.
"Our goal was to facilitate diagnosis," says Ellen Wright Clayton of Vanderbilt University in Nashville, Tennessee, and chair of the panel that drafted the report. "We hope these evidence-based diagnostic criteria provide a new foundation for future research regarding cause and treatment."
Simon Wessely at King's College London welcomes the criteria, but is less convinced by the name-change. "I'm concerned it may add to, not reduce, confusion around this condition," he says.
This article will appear in print under the headline "Fatigue checklist"
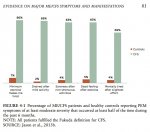
Exacerbation of Pain Following Exertion
Many studies have demonstrated that pain is increased and prolonged after a physical stressor in ME/CFS subjects compared with healthy or sedentary controls. Similar to the evidence base for fatigue, reports of increased pain among ME/CFS subjects are consistent across maximal exercise tests (Davenport et al., 2011a,b; VanNess et al., 2010) and other physical stressors (Black et al., 2005; Nijs et al., 2010). In at least two stud- ies, though, the increase in pain after exertion among ME/CFS subjects was not statistically significant compared with controls (Bazelmans et al., 2005; Kishi et al., 2013).
Simon Wessely at King's College London welcomes the criteria, but is less convinced by the name-change. "I'm concerned it may add to, not reduce, confusion around this condition," he says.
There are many people commenting below this article that they don't like the name.Our lovely David Tuller in the NYT:
http://well.blogs.nytimes.com/2015/02/10/chronic-fatigue-syndrome-gets-a-new-name/?_r=3
From what I recall, there's no limitations specific to ME/SEIDS patients. But there is a blanket statement along the lines of "Don't donate if you're sick".So does the American position differ?
It is a little concerning that Simon is somewhat on board.Translation: "I'm concerned that patients could erroneously believe that they are ill."
If I could leave my home, I'd hand-deliver a copy of the report to the Mayo Clinic.
View attachment 9939
 Yes, that is the spirit. We need to get a hold of the information in this report and USE IT. This means arguing with snide detractors, entrenched deniers, people like Wessely who has caused so much confusion and damage to patients himself. Naturally we are going to get a lot resistance but we must not give up. Let's encourage ourselves and each other to use what we have in this report.
Yes, that is the spirit. We need to get a hold of the information in this report and USE IT. This means arguing with snide detractors, entrenched deniers, people like Wessely who has caused so much confusion and damage to patients himself. Naturally we are going to get a lot resistance but we must not give up. Let's encourage ourselves and each other to use what we have in this report.OMF END ME/CFS said:New Name, New Criteria, Call for more research-IOM Reports today
Today, the Institute of Medicine released a report that recommends a new name for ME/CFS and new clinical diagnostic criteria. This was evidence-based, meaning they listened to experts and reviewed the medical research. The chairman of the report said that there needs to be a lot more work in researching this disease.
The recommended name is “SEID,” short for Systemic Exertion Intolerance Disease. See a report brief here. And you can see the report key facts here.
The new clinical diagnostic criteria requires six months of profound fatigue with a substantial decrease in function, and it also requires post-exertional malaise, unrefreshing sleep and either cognitive dysfunction or orthostatic intolerance. The report includes a new diagnostic algorithm for clinicians to use. Importantly, the report suggests questions physicians can use to determine if a person has the disease.
While this effort has been under much debate, our scientific advisory board director, Ronald W. Davis, PhD, was one of the committee members who worked over a year and a half to ensure patient interests were represented in the end result. He brought the unique perspective of genetics research and personal experience because his son has a severe case of the disease.
"I don't think people understand how horrible this disease is,” Dr. Davis is quoted as saying in a recent Medscape Medical News article. “They don't look that sick. Even my son, who is incredibly debilitated, doesn't look sick." We hope this new name and criteria will make people see the devastation this disease can cause, even if the patients “don’t look sick.”
The IOM reported up to 2.5 million Americans have the disease, yet hundreds of thousands of Americans have the disease but are either undiagnosed or misdiagnosed. This is a global problem with millions affected all over the world with an economic impact estimated at $24 billion annually just in the U.S.
The goal in the report is make it so any doctor can diagnose the disease, a goal we all share. Making the illness part of mainstream medicine will increase research interest.
We will not know the full effect of this change for years, but we are hopeful. As always, we will do all we can to continue our research into biomarkers and treatments. Because we at OMF-Open Medicine Foundation have also been personally touched by this debilitating disease, we want what patients want most of all: a cure that will allow them to return to full vitality.
We want to thank our own Dr. Davis and other experts who served on this committee for giving their time and protecting patient interests when the government and other agencies take initiatives that will affect the patients.
Today, the Institute of Medicine (IOM) released a report of proposed changes to the naming and diagnosis of myalgic encephalomyelitis, more commonly known as chronic fatigue syndrome. Several important recommendations were made that will substantially change both research and clinical practice....
I believe this report represents a very promising move forward in terms of “legitimizing” the disorder. We are now seeing a true push to recognize SEID as an important medical entity, and to train medical professionals to diagnose the disorder. It may take some time to see the true benefits of this move, especially because there are no approved treatments for the diagnosis. However, in the short term, we will likely see a drastic increase in the number of diagnoses made (it is currently severely underdiagnosed), and more exposure for the condition. In the medium term, the move should result in more research funding being devoted to the area....
Sincerely,
Jarred Younger, PhD
Director - Neuroinflammation, Pain and Fatigue Laboratory
Associate Professor, Department of Psychology
Associate Professor, Departments of Anesthesiology and Rheumatology
Just received this from OMF:
There's no cure for mean and stupid.http://www.medscape.com/viewarticle/839532#vp_2
Some of the comments show how this report is no magic wand...
To: CFSAC-L@LIST.NIH.GOV
Statement from Nancy C. Lee, MD, Deputy Assistant Secretary for Health - Women’s Health and Director of the HHS Office on Women’s Health:
The HHS Office on Women’s Health and the other sponsoring agencies* want to thank the Institute of Medicine (IOM) Committee on Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) for its thoughtful analysis in developing this important report. We are pleased with the committee’s recognition of the impact that ME/CFS has on the lives of many Americans. With their recommendation of a streamlined, yet evidence-based set of diagnostic criteria, the IOM committee has taken a critical step toward assisting medical providers in making a diagnosis for those with this serious and debilitating illness.
We are committed to working with our Federal partners, stakeholders, and experts in the field, as well as with the HHS Chronic Fatigue Syndrome Advisory Committee, to reviewthe report’s recommendations and appropriate next steps.
*The Agency for Health Care Research; the Centers for Disease Control and Prevention; the Food and Drug Administration; the National Institutes of Health; and the Social Security Administration.