
Rufous McKinney
Senior Member
- Messages
- 14,502
lactate in the blood and lactate in the brain or muscles is two different things
likely in the lymph and in the spinal fluid,too

lactate in the blood and lactate in the brain or muscles is two different things
I'd be curious where the substantial epidemiological data is for me/cfs In general (are there geographical studies with big enough samples to extrapolate anything useful from , rated by severity ?)Now of course, we should avoid as many toxins in our environment/diet as possible, particularly with CFS. But apart from some obvious exceptions (asbestos and mesothelioma, or cigarettes and lung cancer just to name a couple), the actual epidemiological data suggests that, in general, we are not succumbing to an overload of toxins which results in (or contributes to) CFS.
Lets study the long term effects of micro plastics , chlorpyrifos, atrazine, nanoparticles of metal pollution, etc etc etc before we dismiss them
But there's no way to measure it in the brain. If you're worried about lactate in the muscles, you might try a Vasper, which helps lactate to dissipate more readily.I mean, lactate in the blood and lactate in the brain or muscles is two different things. Obviously if we had pdh complex deficiency u would expect lactate in the blood too, but maybe lower levels could just be in the tissues or cells
No.I'd be curious where the substantial epidemiological data is for me/cfs In general (are there geographical studies with big enough samples to extrapolate anything useful from , rated by severity ?)
They absolutely do.But would it really be outlandish, in context of introducing probably thousands of totally novel chemicals into the environment, to think that some of them probably cause diseases ?
The first time I heard Naviaux speak was at the 2016 United Mitochondrial Disease Foundation Conference. He had done his Cell Danger Response Talk, then researchers gig up and spoke about how they'd found that 75% of pharmaceuticals are toxic to mitochondria. Naviaux claimed the Q&A time, turning to the doctors in the audience and implored them to think about their patients when they prescribed drugs. He said the doctors also needed to be aware of all of the chemicals in their patients' environments and become vocal about cleaning up the planet.Robert naviaux, the me/cfs scientist, has some interesting data about rates of chronic diseases and increased chemicals.
In the paul Cheney seminar above he discusses research measuring it in the brain, via some type of imagingBut there's no way to measure it in the brain. If
In the paul Cheney seminar above he discusses research measuring it in the brain, via some type of imaging
Dr. Younger’s pilot study provides compelling evidence that low-level neuroinflammation – present across a range of brain areas – is a factor in ME/CFS.
The results corroborate previous observations of brain abnormalities, including elevated lactate, and extend findings from MRS studies that were limited to specific regions of the brain.
MRS, a type of MRI scan, provides a non-invasive method for evaluating the types and quantities of chemicals in the brain using 3D images and can give a readout of metabolic changes.
The researchers found that “metabolite and temperature abnormalities were distributed across large portions of the brain” in ME/CFS participants, as compared to controls.
The most significant finding was elevation of choline in the anterior cingulate (ACC) area of the brain on the left side.
Increases in choline are associated with immune cell activation and the authors note that previous research indicates a critical role for the ACC region in cytokine-induced fatigue.
Lactate (a byproduct of glycolysis in an oxygen-limited environment) was found to be increased in a number of brain areas, consistent with brain inflammation and an energy deficit at the cellular level.
Higher average temperatures were observed in five brain areas; the researchers included assessments that showed this finding wasn’t attributable to differences in blood flow or whole-body temperature.
Inflammation requires more metabolic expenditures and three of the five areas also measured increased lactate, suggesting increased metabolism that could be related to neuroinflammation.
Yeah I believe they were not the firstJarred Younger and other researchers have found elevated lactate levels in the brain of ME/CFS patients. Younger used magnetic resonance spectroscopy (MRS).
https://solvecfs.org/jarred-younger/
btw if anyone has any post tbi /concussion treatments besides "xenon " I would love some.
Abstract
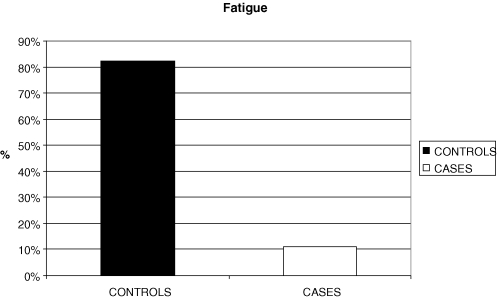
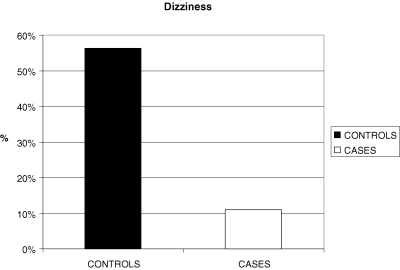
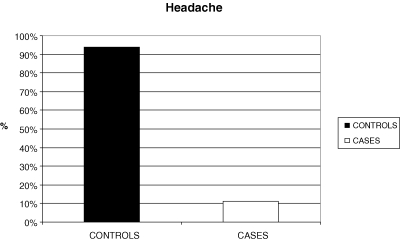
Aim: The complex pathobiology of traumatic brain injury (TBI) offers numerous targets for potential neuroprotective agents. We evaluate the clinical benefit after creatine (Cr) administration in children and adolescents.
Methods: A prospective, randomized, comparative, open- labelled pilot study of the possible neuroprotective effect of Cr was carried out on 39 children and adolescents, aged between 1 and 18 years of age, with TBI. The Cr was administered for 6 months, at a dose of 0.4 g/kg in an oral suspension form every day. For categorical variables, we used the Chi-square test to identify differences between controls and cases. Statistical significance was defined as a p-value <0.05 and not statistically significant if p-value >0.1.
Results: The administration of Cr to children and adolescents with TBI improved results in several parameters, including duration of post traumatic amnesia (PTA), duration of intubation, intensive care unit stay. Significant improvement was recorded in the categories of headache (p<0.001), dizziness (p=0.005) and fatigue (p<0.001), aspects in all patients. No side effects were seen due to Cr administration.
Conclusion: More specific examinations including brain spectroscopy for in vivo evaluation of Cr can be done, in order to draw conclusions for the optimal duration and manner of Cr supply, as well as its possible role for the prevention of TBI complications, in double blind studies.
In the paul Cheney seminar above he discusses research measuring it in the brain, via some type of imaging
Jarred Younger and other researchers have found elevated lactate levels in the brain of ME/CFS patients. Younger used magnetic resonance spectroscopy (MRS).
The nutrients you mention are all mitochondrial nutrients.I can't help but wonder how much of my improvements from coq10, B1, BCAA's etc. is actually from them affecting PDH in the brain.
But we're in a thread about a discussion about a research paper... hence why I think its on topic to bring up research papers that support the flute mella findings. This isn't a thread about someone's personal lactate findingsThis is all fine and well, but most of us do not have access to researchers with these tests. So, we just don't know. I've found it's a lot more useful to solve problems I know I have, which are plenty, than to treat something instead about in a research paper. One can certainly try to extrapolate, but, at best, it's just a guess.
I think it's extremely useful to take research findings and find a way to ones own situation. As there is no standard of care for this disease, it's the only path to wellness - see what can be tested, see what matches, then devise a treatment strategy to normalize the out of whack results. Research to put on a shelf and admire is fabulous, but leads to waiting for 30 years before something usable has been concluded, RCTd and written up as a "standard of care." I don't know about you, but having that all early buttoned up when I'm 90 isn't going to be useful to me. Research is useful to patients if it can be made useful today. It is not optimum, or the way things are typically done, but it yields to results today, before someone is too old to benefit.But we're in a thread about a discussion about a research paper... hence why I think its on topic to bring up research papers that support the flute mella findings. This isn't a thread about someone's personal lactate findings
I'm sure one could extrapolate something useful from these results to clinical treatment, actually, but that's not even the point. Some degree of compartmentalization is useful. Putsuing the empirival reality and results regardless of how inconvenient the application could be is necessary . Translating it to accessible , useful things is a whole other thing.I think it's extremely useful to take research findings and find a way to ones own situation. As there is no standard of care for this disease, it's the only path to wellness - see what can be tested, see what matches, then devise a treatment strategy to normalize the out of whack results. Research to put on a shelf and admire is fabulous, but leads to waiting for 30 years before something usable has been concluded, RCTd and written up as a "standard of care." I don't know about you, but having that all early buttoned up when I'm 90 isn't going to be useful to me. Research is useful to patients if it can be made useful today. It is not optimum, or the way things are typically done, but it yields to results today, before someone is too old to benefit.
If we focused on only the research that is extrapolated easily to practical solutions that are also accessible currently we might not have any research that is valuable at all. I think it's better to compqrtmentalize personal experimentation and research/theory... while we hope that theory and general me/cfs research informs our experimentation, I think it's also important to realize it has valid goals beyond telling us which test to get today, I mean it could lead to a breakthrough in a year.I'm sure one could extrapolate something useful from these results to clinical treatment, actually, but that's not even the point. Some degree of compartmentalization is useful. Putsuing the empirival reality and results regardless of how inconvenient the application could be is necessary . Translating it to accessible , useful things is a whole other thing.
Just bc a test cant be done for most people doesnt mean it isn't valuable research. In the least. In fact, I sort of disagree with how the open medicine foundation is focused on finding an accessible and affordable test and treatment--that is limiting the possibilities before even finding them. If we had a genuinely widely validated test and treatment that was costly, we could make it accessible/affordable. But what if we miss out on something like that bc of circumscribing what it should be beforehand rather than following the science?
Fluge and Mella Found a Pyruvate Dehydrogenase Impairment in ME/CFS: Does This Really Explain ME/CFS?
A new argument suggests pyruvate dehydrogenase (PDH) impairment may not be a candidate for the underlying cause of ME/CFS.
In Fluge and Mella's 2016 metabolomic study, they found impaired pyruvate dehydrogenase function in ME/CFS, and it has been speculated this might be the cause of the apparent energy metabolism dysfunction of this disease — a dysfunction which causes fatigue and other ME/CFS symptoms.
@Kalliope posted a link to a pertinent argument raised by Dr Yngve Thomas Bliksrud in the Journal of the Norwegian Medical Association (Google translation here), in which Dr Bliksrud discusses Fluge and Mella's results, and points out that:
Dr Bliksrud says the fact that patients with genetic PDH deficiency diseases do not generally experience fatigue suggests that the PDH impairment found by Fluge and Mella may not be the cause of ME/CFS.
But conceivably Fluge and Mella's PDH impairment may be a consequence of some other more fundamental energy metabolism dysfunction in ME/CFS, rather than the actual cause of the ME/CFS energy dysfunction.
So what might be the real underlying energy metabolism dysfunction that both causes ME/CFS, and gives rise to this PDH impairment?
One possibility is comes from the 2009 energy metabolism studies of Myhill, Booth and McLaren-Howard where they found that the mitochondrial translocator protein is blocked in ME/CFS, and posited this causes an energy metabolism blockage. (Note though that translocator protein blockage was not the only energy metabolism impairment found by Myhill et al in ME/CFS).
Myhill, Booth and McLaren-Howard point out that if the translocator protein is blocked, then pyruvate dehydrogenase automatically becomes inhibited. See their 2012 study:
So it's possible that the PDH inhibition found by Fluge and Mella may be a consequence of the translocator protein blockage found by Myhill, Booth and McLaren-Howard in ME/CFS patients. Or may be a consequence of some other as yet undiscovered energy metabolism dysfunction.
Note that Myhill et al use the term "translocator protein" to refer to the adenine nucleotide translocator (ANT).
Also of relevance: Enterovirus-Induced ANT Autoantibodies: the Cause of ME/CFS? Could autoantibodies that target ANT (the mitochondria translocator protein) be the cause of ME/CFS? Such ANT autoantibodies would certain fit in with Fluge and Mella's finding that there is "something in the serum" of ME/CFS patients that is causing the energy metabolism blockage (autoantibodies are found in the blood serum).