We just finished another bad day in the US, with COVID-19 deaths jumping by 1321 for a total of 7392. Here are the latest historical charts from Worldometer:
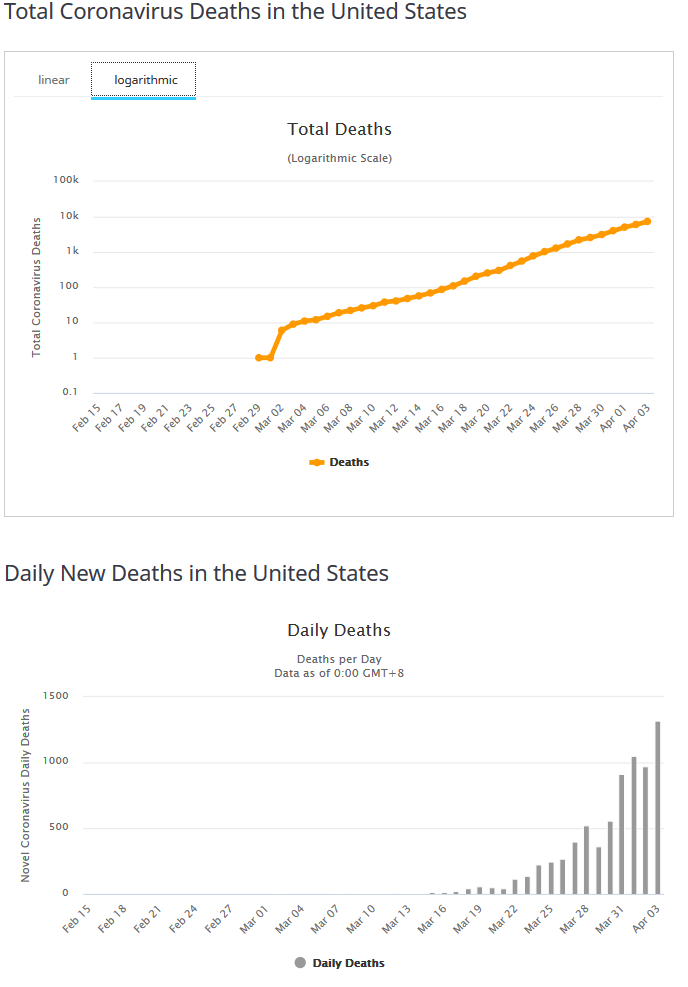
Note that I have selected the logarithmic scale for the first chart. To the extent that that data falls along a straight line, it means that growth is proceeding at a steady exponential rate. If you put a straightedge connecting March 2nd to April 2nd, you'll see that it fits the data very well. On average, since March 2nd, the total deaths have been increasing by a factor of 10 every 10 1/3 days. This means that after three cycles - 31 days - the total number of deaths has increased by a factor of 1000. Sure enough, March 2nd had 6 deaths, while April 2nd had 6071.
For those who don't think that 6071 is a big deal, if the line continues at its present slope, the total deaths for April 12th will be about 60,000, and the total deaths for April 23rd would be about 600,000 - far above official projections. Hopefully, the mitigation procedures will be having much more of an effect by then, and we won't get anywhere near 600,000. On the other hand, if what we do isn't working, and we do see around 600,000 or so deaths by April 23rd, the next 10-day period ending on May 3 could see total deaths rise into the millions. A factor of 10 growth resulting in total deaths of 6 million would be unlikely in the extreme, as by this time there would be many forces working to level the curve.
BTW, the numbers for the UK are even worse. In the 30-day period ending today, total deaths rose from one to 3605 - almost exactly half the total deaths as in the US. Considering that the UK has only a fifth of the population of the US, this bodes poorly for total mortality as a percentage of population in the UK.
If these numbers look outrageous to anyone, please review the video in the first post in this thread. It is in the nature of exponential growth to appear to be going nowhere for a long time, and then suddenly become totally overwhelming.
For those who don't think that 6071 is a big deal, if the line continues at its present slope, the total deaths for April 12th will be about 60,000, and the total deaths for April 23rd would be about 600,000 - far above official projections. Hopefully, the mitigation procedures will be having much more of an effect by then, and we won't get anywhere near 600,000. On the other hand, if what we do isn't working, and we do see around 600,000 or so deaths by April 23rd, the next 10-day period ending on May 3 could see total deaths rise into the millions. A factor of 10 growth resulting in total deaths of 6 million would be unlikely in the extreme, as by this time there would be many forces working to level the curve.
BTW, the numbers for the UK are even worse. In the 30-day period ending today, total deaths rose from one to 3605 - almost exactly half the total deaths as in the US. Considering that the UK has only a fifth of the population of the US, this bodes poorly for total mortality as a percentage of population in the UK.
If these numbers look outrageous to anyone, please review the video in the first post in this thread. It is in the nature of exponential growth to appear to be going nowhere for a long time, and then suddenly become totally overwhelming.
 . Although it is very scary to read, knowledge is power.
. Although it is very scary to read, knowledge is power.