Hi.
This may take a bit to explain. But it relates to Chris Armstrong's presentation at Stanford. The one in which he explained that pwme/cfs seem to be locked into a vicious cycle.
The steps are:
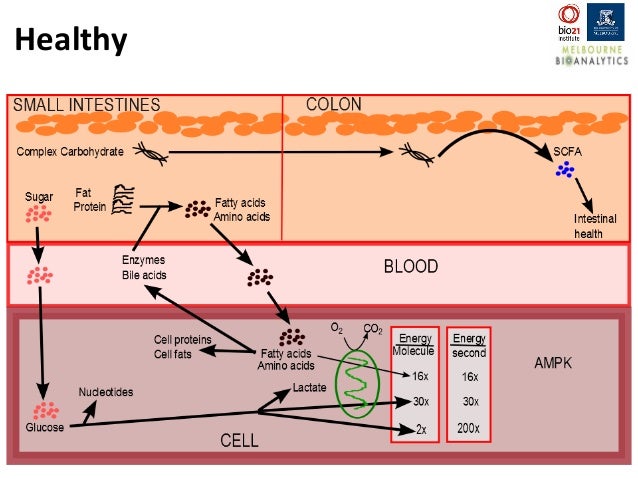
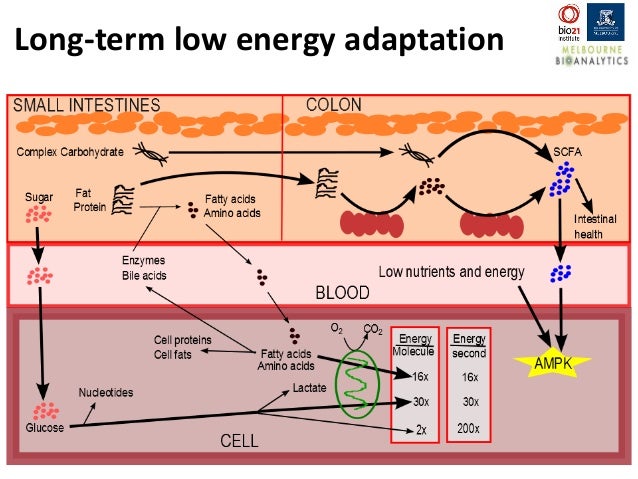
1) we do not have enough ATP so we switch on AMP kinase;
2) which puts our cells into an energy efficient mode that favours the use of lipids and proteins for energy;
3) which means that they no longer have those lipids and proteins available for making enzymes and bile;
4)which means that fats and proteins are not properly digested in the small intestine and pass through to the colon;
5) where they change the balance of our gut bacteria leading to an increase in production of Short Chain Fatty Acids;
6)which in turn trigger AMPK, reinforcing the cycle.
And we do in a sense seem to have a kit to deal with this.
1) Betaine HCL plus pepsin allow us to emulate the acid and pepsin production and release of normal people breaking proteins into peptides.
2) Creon or another source of animal derived pancreatic enzymes can then break these proteins into small oligopeptides
3) ox bile to break fat down into manageable globules and lipases (in the Creon) to break them down into monoglycerides and free fatty acids.
(The creon also works on carbohydrates too but Armstrong was focussed on proteins and lipids, so I have too.)
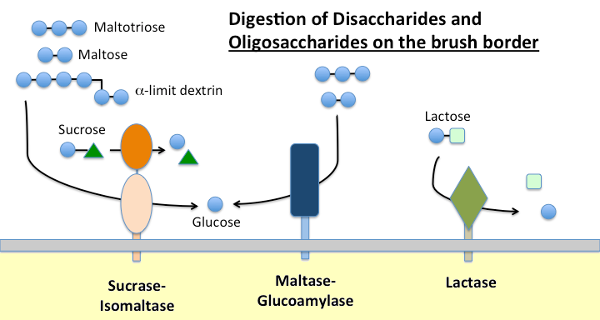
I think that there is a problem though. We can kind of approximate a working stomach and pancreas and gall bladder but we are not replicating the brush border enzymes that activate some of the pancreatic enzymes and turn the oligopeptides into the amino acids, dipeptides and tripeptides that we can absorb.
(For lipids I think that the Creon and ox bile should be enough to do the job.)
I got to thinking about this because I was playing around with Oral Rehydration Solutions to try to reduce the severity of my PoTS.
In reading the ORS research I found that there are the usual sodium, potassium, glucose and citrate or bicarbonate solutions and others that use cooked cereal flours in the place of glucose. It seems like the cereal had an advantage when trying to rehydrate people with diarrhoeal infections that did not damage the gut, but were a disadvantage for those with infections that had damaged the gut.
The trick to ORS is glucose sodium symporters. These transport equal numbers of sodium ions and glucose molecules into the cells and create the osmotic pressure that brings the water across from the small intestine into the body. The cereal solutions uses brush border enzymes to break the carbohydrates into the glucose needed to make the trick work without increasing the osmolarity of the solution.
When I tried the cereal solutions on myself I found that they were indistinguishable from ORS minus glucose. Which is to say that they were of little use. I conclude from that rather unprofessional n=1 experiment (2 litres solution on 2 days) that they did not work for me, But had to read and think for a few weeks before it occurred to me that this might be because my brush border enzymes are not being produced, or not being produced in sufficient quantities.
The normal ORS really helps with the PoTS but I have issues with having too much glucose - it makes me feel ill, makes it hard to sleep, it feels a bit like being drunk.
So it occurred to me that it should be possible to use the same principle as ORS with sodium dependent amino transporters. So I tried it with whey protein and like the cereal based ORS it had no effect. (Even when I took it with Betaine hcl, Pepsin and Creon).
Which lead me to read about brush border enzymes and here.
My hope with the Betaine HCL + pepsin + oxbile +Creon combination was to digest and absorb the nutrients my body needs and to provide the right substrates to grow the right bacteria and get rid of the dysbiosis that is characteristic of ME/CFS.
I think Chris Armstrong's presentation underlines the importance of sorting out this dysbosis.
And the current kit has improved things, but if I am right it cannot get someone all the way.
What I am wondering is if people who have a better handle on the biology and biochemistry are aware of exogenous sources of enzymes that can fill the role of brush border enzymes.
Or if taking amino acids (glutamine and luecine perhaps) or something of the sort might be able to get those cells on the brush border to down regulate AMPK or at least get the lipids and aminos needed for making the brush border enzymes.
Or if I am just very very wrong, and have misunderstood something important.
In reading up on the above I have chiefly relied on this site for info on digestion.
http://www.vivo.colostate.edu/hbooks/pathphys/digestion/smallgut/index.html
This may take a bit to explain. But it relates to Chris Armstrong's presentation at Stanford. The one in which he explained that pwme/cfs seem to be locked into a vicious cycle.
The steps are:
1) we do not have enough ATP so we switch on AMP kinase;
2) which puts our cells into an energy efficient mode that favours the use of lipids and proteins for energy;
3) which means that they no longer have those lipids and proteins available for making enzymes and bile;
4)which means that fats and proteins are not properly digested in the small intestine and pass through to the colon;
5) where they change the balance of our gut bacteria leading to an increase in production of Short Chain Fatty Acids;
6)which in turn trigger AMPK, reinforcing the cycle.
And we do in a sense seem to have a kit to deal with this.
1) Betaine HCL plus pepsin allow us to emulate the acid and pepsin production and release of normal people breaking proteins into peptides.
2) Creon or another source of animal derived pancreatic enzymes can then break these proteins into small oligopeptides
3) ox bile to break fat down into manageable globules and lipases (in the Creon) to break them down into monoglycerides and free fatty acids.
(The creon also works on carbohydrates too but Armstrong was focussed on proteins and lipids, so I have too.)
I think that there is a problem though. We can kind of approximate a working stomach and pancreas and gall bladder but we are not replicating the brush border enzymes that activate some of the pancreatic enzymes and turn the oligopeptides into the amino acids, dipeptides and tripeptides that we can absorb.
(For lipids I think that the Creon and ox bile should be enough to do the job.)
I got to thinking about this because I was playing around with Oral Rehydration Solutions to try to reduce the severity of my PoTS.
In reading the ORS research I found that there are the usual sodium, potassium, glucose and citrate or bicarbonate solutions and others that use cooked cereal flours in the place of glucose. It seems like the cereal had an advantage when trying to rehydrate people with diarrhoeal infections that did not damage the gut, but were a disadvantage for those with infections that had damaged the gut.
The trick to ORS is glucose sodium symporters. These transport equal numbers of sodium ions and glucose molecules into the cells and create the osmotic pressure that brings the water across from the small intestine into the body. The cereal solutions uses brush border enzymes to break the carbohydrates into the glucose needed to make the trick work without increasing the osmolarity of the solution.
When I tried the cereal solutions on myself I found that they were indistinguishable from ORS minus glucose. Which is to say that they were of little use. I conclude from that rather unprofessional n=1 experiment (2 litres solution on 2 days) that they did not work for me, But had to read and think for a few weeks before it occurred to me that this might be because my brush border enzymes are not being produced, or not being produced in sufficient quantities.
The normal ORS really helps with the PoTS but I have issues with having too much glucose - it makes me feel ill, makes it hard to sleep, it feels a bit like being drunk.
So it occurred to me that it should be possible to use the same principle as ORS with sodium dependent amino transporters. So I tried it with whey protein and like the cereal based ORS it had no effect. (Even when I took it with Betaine hcl, Pepsin and Creon).
Which lead me to read about brush border enzymes and here.
My hope with the Betaine HCL + pepsin + oxbile +Creon combination was to digest and absorb the nutrients my body needs and to provide the right substrates to grow the right bacteria and get rid of the dysbiosis that is characteristic of ME/CFS.
I think Chris Armstrong's presentation underlines the importance of sorting out this dysbosis.
And the current kit has improved things, but if I am right it cannot get someone all the way.
What I am wondering is if people who have a better handle on the biology and biochemistry are aware of exogenous sources of enzymes that can fill the role of brush border enzymes.
Or if taking amino acids (glutamine and luecine perhaps) or something of the sort might be able to get those cells on the brush border to down regulate AMPK or at least get the lipids and aminos needed for making the brush border enzymes.
Or if I am just very very wrong, and have misunderstood something important.
In reading up on the above I have chiefly relied on this site for info on digestion.
http://www.vivo.colostate.edu/hbooks/pathphys/digestion/smallgut/index.html