No, it's only compound heterozygous if the mutations are on different strands. It's literally impossible to figure that out from your 23andMe results alone. If both mutations are from the same parent, you aren't compound heterozygous and it's equivalent to just being MTHFR C677T +/-. So there's only a 50% chance that you're compound heterozygous.A person's 23andme raw data when uploaded to an online service such as "Promethease" or "Genetic Genie"does indeed tell you your MTHFR status. Mine shows I am "Compound Heterozygous" using just my own raw data alone as neither of my parents have been tested.

-

Welcome to Phoenix Rising!
Created in 2008, Phoenix Rising is the largest and oldest forum dedicated to furthering the understanding of, and finding treatments for, complex chronic illnesses such as chronic fatigue syndrome (ME/CFS), fibromyalgia, long COVID, postural orthostatic tachycardia syndrome (POTS), mast cell activation syndrome (MCAS), and allied diseases.
To become a member, simply click the Register button at the top right.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
No libido since forever, A1298C positive.
- Thread starter pab
- Start date
Dufresne
almost there...
- Messages
- 1,039
- Location
- Laurentians, Quebec
No, I don't have ME/CFS. I may not have energy levels you'd expect from a 27yo but I'm doing pretty well. I'm working in a fast-paced environment which requires a lot of multitasking and being cognitively sharp and I'm doing well. Trying to be at least 4 times a week at the gym, have an over-average physique (though it's quite obvious I need more time and efforts than others to build muscle/lose fat).
Although no obvious event or situation, at least that I remember, I'd say the most probable answer would be: took accutane. There is quite a few folks reporting similar side effects to mine. However, it seems that some of them get better with time or some supplementation/drugs. I don't.
Been eating super healthy (no processed food since many years), alcohol twice a year max, no drugs, no nicotine, sleeping 7-8 hours.
So did you notice your libido drop while you were taking Accutane? In the following article they cite a Spanish study that suggests the sexual side effects to the drug are far more common than thought.
http://rxisk.org/accutane-30-years-of-trading-our-sex-lives-for-clear-skin/
How long ago did you stop taking the drug?
Trying to be at least 4 times a week at the gym, have an over-average physique (though it's quite obvious I need more time and efforts than others to build muscle/lose fat).
Difficulty with both building muscle and losing fat, coupled with the libido issue could suggest there's a problem with your androgen system. The following is from the article linked above.
Studies demonstrate that isotretinoin significantly disrupts normal endocrine function. IGF-1, pituitary hormones, 5-alpha and 3-alpha reduced steroids, and androgen receptor levels have been observed to be significantly decreased in patients as a result of isotretinoin treatment. Hormonal antagonism elicited by isotretinoin is considered to be one of the ways it helps in acne. Hormonal antagonism is also believed by many in our patient group to be a likely explanation of the sexual side effects they experienced as a result of taking this drug. But it’s difficult for anyone to help given the current limited understanding of isotretinoin’s full range of biological effects.
A medical hypothesis published in 2009 proposed that long-term side effects associated with isotretinoin, including erectile dysfunction, may be the end result of persistent modifications to mechanisms which control gene expression (4). If true, this would indeed explain the enduring nature of sexual symptoms which emerged during isotretinoin treatment.
I found a lengthy thread on an acne forum that might have some decent info about this problem.
http://www.acne.org/messageboard/topic/295030-repairing-the-long-term-damage-from-accutane/?page=1
@Dufresne
I'm well aware about accutan and sexual sides. Thing is there in no explanation why and how to overcome them. Everybody seems to be getting their "own" set of sides which require different apporach.
I know this forum you mention, been posting there from time to time.
Androgen connection has been discussed to death. I took accutane some 10 years ago and a couple years after, when I did my first ever test of free testosterone it came terribly low (as opposed to normal score of total testosterone).
Took clomifene (clomid) which resulted in a sky high free testosterone score and this had absolutely no impact on my sexual life. Another doctor gave me testosteron injections which didnt't prove to be helpful whatsover.
At the moment my androgens are ok, same with other hormones.
These experiments sort of confirm that the problem is more general and some mechanisms are not doing their job/something is obstructing the normal pathways.
As far as I know guys who did overcome their sexual sides:
1) two-three of them took marijuana oil (RSO). In my case it caused terrible anxiety problems.
2) 1 guy claims he cleansed his body with raw food diet. Tried and tested for over a year. No results.
3) there is someone claiming it all improved with time. I'm about to hit the 10 year of this misery. Was so disinterested in sex today that's couldnt stay erect despite my sexy lady being in a mood
4) some guys get sexual drive after taking dopamine agonists. Tried with two, one being cabergoline - nothing happened after I've taken it.
5) similar problems are known to happen after finasteride/propecia. Some folks get better with androgens/dht (not my case), some via improving gut flora (working on it, seems not to be my case though, no slightest improvement as yet), some with fasting and cleanses.
Among the theories which are discussed in the community there was the one about downregulated Fox0 (http://www.allthingsmale.com/community/threads/growth-factor-targeting-and-foxo-genes.21669/)
Nothing useful came out of this as yet, sadly.
edit: this pdf briefly sums up the research about sexual side effects of Accutane: https://www.docdroid.net/Lx9ecb2/accutane-link-with-ed-sexual-dysfunction.docx.html
I'm well aware about accutan and sexual sides. Thing is there in no explanation why and how to overcome them. Everybody seems to be getting their "own" set of sides which require different apporach.
I know this forum you mention, been posting there from time to time.
Androgen connection has been discussed to death. I took accutane some 10 years ago and a couple years after, when I did my first ever test of free testosterone it came terribly low (as opposed to normal score of total testosterone).
Took clomifene (clomid) which resulted in a sky high free testosterone score and this had absolutely no impact on my sexual life. Another doctor gave me testosteron injections which didnt't prove to be helpful whatsover.
At the moment my androgens are ok, same with other hormones.
These experiments sort of confirm that the problem is more general and some mechanisms are not doing their job/something is obstructing the normal pathways.
As far as I know guys who did overcome their sexual sides:
1) two-three of them took marijuana oil (RSO). In my case it caused terrible anxiety problems.
2) 1 guy claims he cleansed his body with raw food diet. Tried and tested for over a year. No results.
3) there is someone claiming it all improved with time. I'm about to hit the 10 year of this misery. Was so disinterested in sex today that's couldnt stay erect despite my sexy lady being in a mood
4) some guys get sexual drive after taking dopamine agonists. Tried with two, one being cabergoline - nothing happened after I've taken it.
5) similar problems are known to happen after finasteride/propecia. Some folks get better with androgens/dht (not my case), some via improving gut flora (working on it, seems not to be my case though, no slightest improvement as yet), some with fasting and cleanses.
Among the theories which are discussed in the community there was the one about downregulated Fox0 (http://www.allthingsmale.com/community/threads/growth-factor-targeting-and-foxo-genes.21669/)
Nothing useful came out of this as yet, sadly.
edit: this pdf briefly sums up the research about sexual side effects of Accutane: https://www.docdroid.net/Lx9ecb2/accutane-link-with-ed-sexual-dysfunction.docx.html
Last edited:
TrixieStix
Senior Member
- Messages
- 539
No, it's only compound heterozygous if the mutations are on different strands. It's literally impossible to figure that out from your 23andMe results alone. If both mutations are from the same parent, you aren't compound heterozygous and it's equivalent to just being MTHFR C677T +/-. So there's only a 50% chance that you're compound heterozygous.
I've never seen any reference to "compound heterozygous" on sites discussing mthfr stating that it means that the mutations must be are on the same strand. The way it is used in popular mthfr discourse is to simply mean having one mutation on each snp.
If you have a link to something stating that they must be on the same strand in order to be considered "compound heterozygous" I'd love to see it. But I've never once seen it defined or used that way.
Those types of sites tend thrive on grossly exaggerating claims, and usually have no apparent knowledge of genetics. They simply repeat claims, usually originating from Yasko, who has been notoriously wrong about pretty much everything.I've never seen any reference to "compound heterozygous" on sites discussing mthfr stating that it means that the mutations must be are on the same strand.
For a bit of a more in-depth explanation: a lot of diseases are recessive, meaning the gene has to have a fault on both strands. If someone has a normal heterozygous mutation, even for a deadly disease, it doesn't matter, because they also have another strand which is completely normal. A compound heterozygous situation arises when there are two different mutations, but one being on each strand. Then there is no normal strand to maintain normal function - both strands are faulty.
http://www.medicinenet.com/script/main/art.asp?articlekey=33675If you have a link to something stating that they must be on the same strand in order to be considered "compound heterozygous" I'd love to see it. But I've never once seen it defined or used that way.
Or any basic genetics course or textbook.
TrixieStix
Senior Member
- Messages
- 539
Those types of sites tend thrive on grossly exaggerating claims, and usually have no apparent knowledge of genetics. They simply repeat claims, usually originating from Yasko, who has been notoriously wrong about pretty much everything.
FYI I'm not claiming that your wrong. When I first learned about the MTHFR thing years ago I had so much trouble finding anything from reputable medical sources refuting claims made by people such as Yasko & Dr. Ben. In my gut I knew right away there was no way their claims could all be true. Then I finally happened upon an article about the Homocysteine thing and I decided for me getting that checked would suffice for me.
I hadn't thought about MTHFR for a few years and I see there are now finally some web sites, articles online criticizing the MTHFR hype.
https://www.sciencebasedmedicine.org/dubious-mthfr-genetic-mutation-testing/
http://www.skepticalraptor.com/skep...utations-are-the-root-of-all-health-problems/
https://drmelthomson.wordpress.com/tag/quackery/
Last edited:
FYI I'm not claiming that your wrong
But you are nevertheless questioning a fundamental genetic concept which would be encountered if you consulted any source of basic genetic information. It's your sources that are wanting, not the concept.
Last edited:
TrixieStix
Senior Member
- Messages
- 539
I was only stating that I am considered "compound heterozygous" according to the way the term is defined in current MTHFR discourse.But you are nevertheless questioning a fundamental genetic concept which would be encountered if you consulted any source of basic genetic information. It's your sources that are wanting, not the concept.
That the term is defined incorrectly by the MTHFR online community is another issue. It doesn't change the fact that they define the term as they do.
That the term is defined incorrectly by the MTHFR online community is another issue. It doesn't change the fact that they define the term as they do.
Who cares how they define it - they are wrong (as they are about many other things). You seem reluctant to accept this.
Dufresne
almost there...
- Messages
- 1,039
- Location
- Laurentians, Quebec
@Dufresne
Androgen connection has been discussed to death. I took accutane some 10 years ago and a couple years after, when I did my first ever test of free testosterone it came terribly low (as opposed to normal score of total testosterone).
Took clomifene (clomid) which resulted in a sky high free testosterone score and this had absolutely no impact on my sexual life. Another doctor gave me testosteron injections which didnt't prove to be helpful whatsover.
At the moment my androgens are ok, same with other hormones.
These experiments sort of confirm that the problem is more general and some mechanisms are not doing their job/something is obstructing the normal pathways.
Yeah, I was thinking more along the lines of a problem with androgen receptors.
My libido has always been low-normal due to my illness, and at times has been virtually nonexistent. I've also been inconvenienced by sexual side effects of medications. I know how frustrating it can be and I can only imagine how you feel about it after such a period of time.
Perhaps trying reputed aphrodisiacs would be a good way to go. It might provide some relief and/or shed some light on the nature of the problem. The one drug that got my libido going like gangbusters was GHB. I don't think it's understood how this drug functions as an aphrodisiac, but many who've tried it experience this effect.
The one drug that got my libido going like gangbusters was GHB. I don't think it's understood how this drug functions as an aphrodisiac, but many who've tried it experience this effect.
Hm...Where do you get GHP from? Don't think it can be obtained legally where I live...
@Glycon @alicec @hixxy @Valentijn
So I got:
MethylB12 - Enzymatic Therapy B12 Infusion, sublingual 1 mg
Methylfolate - Solgar Metafolin (called folate on bottle), 800 microgram tablet
AdenosylB12 - Source Naturals Dibencozide, sublingual 10 mg.
Source Naturals sublingual Flavin Mononucletide
I started slowly and I didn't feel any different than normal. After I increased the dose I noticed that I was getting more and more depressed and anti-social. Once I've given up, I'm in a good mood again.
What do you reckon? What does it tell about me?
After I increased the dose I noticed that I was getting more and more depressed and anti-social. Once I've given up, I'm in a good mood again.
Well at least something happened, even if it didn't work out as you might have hoped.
It sounds to me like you are running out of folate.
Once these B12 pathways open up and start working there can be a large demand placed on various nutrients which quickly become depleted.
Freddd, who has reported most on this issue, has described it in terms of refeeding syndrome. About 3 days after the pathways start functioning with an initial favourable response, there is a marked decline. In starving people being refed, this is sometimes so serious that death results.
The two nutrients most implicated in this immediate response appear to be potassium and folate (potassium particularly so for starvation victims). With time, trace mineral depletion may be a big issue also.
In the post I linked, Freddd describes various symptoms that might be encountered. In my experience it can sometimes be difficult to work out if you need potassium or folate. You just need to try both and see which you respond to, though depression sounds much more like folate.
Needs can change also and it can be a very rocky pathway trying to get things to run more smoothly.
I suggest you try again with the dose of B12 that seemed to be doing something but with 3-4 times as much folate as previously. Spread the folate over 3-4 doses and be prepared to take a lot more. Don't be surprised if you have an almost insatiable need - just keep taking more until the symptoms subside. Eventually you will stabilise on a dose. After that, increasing B12 further is not likely to further increase need for folate.
Have some potassium on hand in case that becomes an issue also.
If you do experience the extremely high folate need don't panic - just go with it at first to help sort out what is and is not working for you. People on PR (including myself) have taken 40-50 mg folate daily for a time. The only thing it will hurt is your pocket.
Effectively making active B2 can help reduce the need for folate, but this too can be difficult. I linked a thread in an earlier post which discusses this.
Using the sublingual FMN will help overcome difficulties in the first stage of formation of the active vitamin (riboflavin > FMN > FAD), and you need molybdenum to get the second stage working.
None of these nutrients should be taken in large amounts in isolation. Have a look at some of the links in my earlier post to get an idea of the range of basic nutrients you may need to supplement, especially all the B vitamins, minerals and trace minerals, fatty acids, basic antioxidants, etc. Freddd used SAMe and TMG also though personally I could never see the point of these.
Many of these nutrients can be helpful in people who have the range of metabolic derangements that seem to prevail in ME/CFS.
Your case is presumably a bit different but I think the same principle applies. It may well be B12 and folate which is driving the response but many other things need to be in place for the whole system to work.
Gondwanaland
Senior Member
- Messages
- 5,095
Have you tried K2-MK4?What I tried to tell in my first post was that nothing and I tried almost everything (suppements, herbs, rx stuff) helps with my libido. Ate tons of zinc, ashwaganda and plethora of other stuff. Nothing can give me even the slightest sexual drive... Clearly something got "switched off" and no-one knows what and how to revert it.
Dufresne
almost there...
- Messages
- 1,039
- Location
- Laurentians, Quebec
Hm...Where do you get GHP from? Don't think it can be obtained legally where I live...
One can obtain GHB legally in many countries, albeit at an exorbitant price, as the pharmaceutical "Xyrem".
Baclofen also works similarly as an aphrodisiac for some, but to a lesser extent.
hi
@Glycon @alicec @hixxy @Valentijn @Dufresene
I'm 1,5 years after this thread was created. Still don't have any libido.
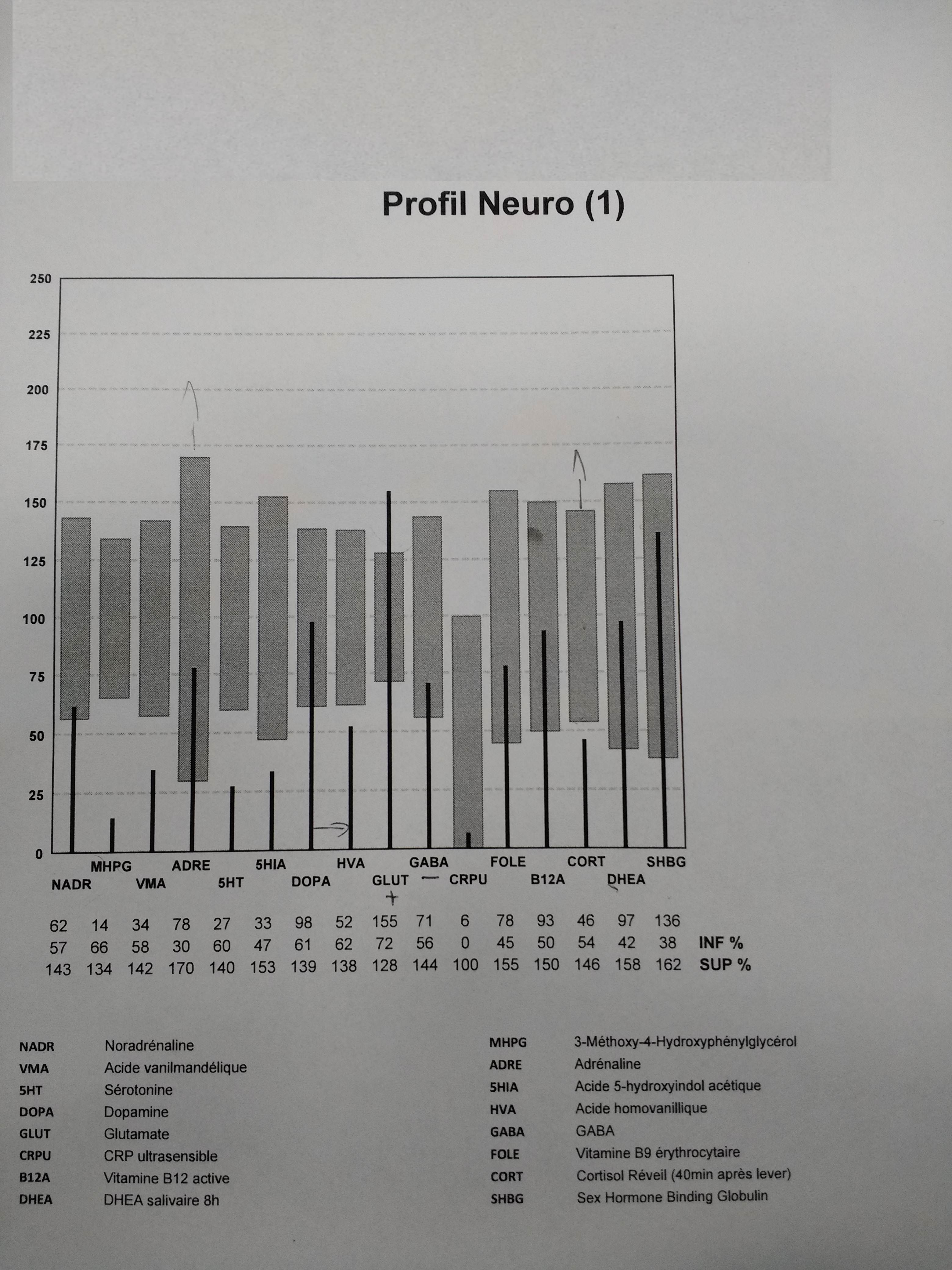
Just got my neuro results however.
Where do I go from there? It seems that noradrenalin metabolites are extremely low. Serotonin and its metabolite is pathetic. Dopamine seems to be alright but the metabolite is extremely low.
Any suggestions on what to do now are more than welcome.
@Glycon @alicec @hixxy @Valentijn @Dufresene
I'm 1,5 years after this thread was created. Still don't have any libido.
Just got my neuro results however.
Where do I go from there? It seems that noradrenalin metabolites are extremely low. Serotonin and its metabolite is pathetic. Dopamine seems to be alright but the metabolite is extremely low.
Any suggestions on what to do now are more than welcome.
Gondwanaland
Senior Member
- Messages
- 5,095
Take a look at the reviews on L-Histidine on AmazonAny suggestions on what to do now are more than welcome.
Critterina
Senior Member
- Messages
- 1,238
- Location
- Arizona, USA
@pab, Doesn't the healthcare practitioner who ordered the test have some suggestions for you?