In response to Dr Robert Jakob's comment, yesterday, via the Proposal Mechanism:
work is still progressing to identify the correct place in the new structures of ICD-11
Robert Jakob, WHO 2017-Mar-10 - 16:05 UTC
http://apps.who.int/classifications...lGroupId=e3426560-b6e4-4c94-b0c8-ba25fabe66fa
Comment
Suzy Chapman 2017-Mar-11 - 13:25 UTC
Thank you, Dr Jakob, for this status update at March 10, 2017.
I note that ICD-10 concept title,
R53 Malaise and fatigue is replaced for ICD-11 Beta with concept title,
Fatigue.
I further note that for ICD-11 Beta,
Fatigue is primary parented under
General symptoms and secondary parented to proposed grouping,
"Symptoms or signs involving motivation or energy."
Re Exclusions: In ICD-10 Volume 1: Tabular List, under
Malaise and fatigue there is an Excl. for
"fatigue syndrome (F48.0)" and also for
"fatigue syndrome: • postviral (G93.3)."
It is not unreasonable, then, to propose that for ICD-11, consideration might also be given to adding exclusions for the G93.3 legacy entities under
Fatigue.
I have been advised by WHO's Linda Best that
"exclusion terms must exist in the classification as entities to enable linking" - a convention that I was unaware of when submitting the proposal for exclusions for the G93.3 legacy entities under
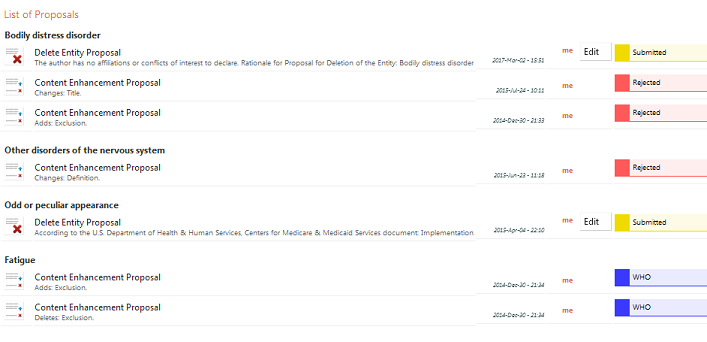
Bodily distress disorder (submitted on December 30, 2014; Rejected on November 15, 2016) and also when submitting the proposal for exclusions for the G93.3 legacy entities under
Fatigue (submitted on December 30, 2014; Status changed to "WHO team is studying the proposal. Editing the proposal is not allowed" on June 19, 2015)
These submissions for exclusions had been informed by the guidance contained within the Content Model Reference Guide ICD-11 Revision, World Health Organization Geneva, 2011.
The number, type and application of exclusions for ICD-11 has been under discussion since 2014. I rely here on the discussion at point 10.5 of Summary Report, Third Meeting of the JLMMS Task Force Cologne, Germany, 11-14 April 2016 [1].
If it is the case that principles for the application of exclusions in ICD-11 have evolved since publication of the Content Model Reference Guide, there is currently no up to date public domain guidance for stakeholders to inform the preparation of proposals or the submission of comments on proposals. A guideline for stakeholder consumption clarifying the current principles for the number, type and application of exclusions would be welcomed.
Re Entity terminology: The Written Response provided on March 7, 2017 by Lord O'Shaughnessy to a Parliamentary Written Question tabled by the Countess of Mar, on February 27, 2017 stated:
"The WHO has also confirmed that the proposal submitted for chronic fatigue is currently with the relevant groups of the organisation to consider the scientifically-based placement of this condition in the classification. This will be included in the next version of ICD-11 to be released on 4 April 2017 for field testing."
This statement has resulted in a good deal of unnecessary confusion. It is not clear whose proposal is being referred to; that is, whether it refers to a proposal submitted by TAG Neurology, or by another TAG, or by another party; or whether it refers to a proposal which I have submitted.
It would be helpful if this point could be clarified.
The Parliamentary statement has also resulted in confusion due to the terminology used. There is no
"chronic fatigue" entity in ICD-10 and no
"chronic fatigue" entity in the public version of the ICD-11 Beta drafting platform (unless TAG Neurology is proposing to add a new entity called,
"chronic fatigue").
As you know, there was a
"Fatigue syndrome" inclusion under ICD-10's,
F48.0 Neurasthenia. But for ICD-11,
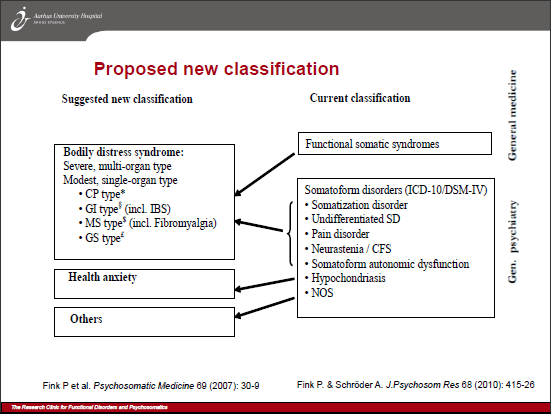
Neurasthenia is retired and has been subsumed by a single, proposed new entity,
Bodily distress disorder, which also subsumes and replaces all the ICD-10 F45.0-F45.9 somatoform disorders, with the exception of Hypochondriasis [2][3]. I note that an exclusion for
bodily distress disorder has been inserted under
Fatigue.
The proposals I submitted in December 2014 were for exclusions for the specific ICD-10 (G93.3) legacy entities:
Postviral fatigue syndrome;
Benign myalgic encephalomyelitis; and
Chronic fatigue syndrome, which are all currently unaccounted for within the public version of the Beta platform.
I have made no proposals in relation to
"chronic fatigue."
Likewise, my letters to the Joint Task Force of February 6, 22 and 23 were in relation to the specific ICD-10 (G93.3) legacy entities:
Postviral fatigue syndrome;
Benign myalgic encephalomyelitis; and
Chronic fatigue syndrome.
There is no context within ICD-10 and ICD-11 in which to place the term
"chronic fatigue." I would suggest, therefore, that it order to avoid confusion the specific ICD-10 (G93.3) legacy terms are referenced.
Re Deadlines: The Written Response provided on March 7, 2017 by Lord O'Shaughnessy stated:
"The WHO has confirmed that the latest version of the 11th Revision of the International Classification of Diseases (ICD-11) includes the Topic Advisory Group for Neurology’s proposals."
This statement also lacks clarity. It is not clear what the "latest version" of ICD-11 refers to. There are certainly no relevant proposals from TAG Neurology in the public version of the Beta, as it stands this week.
Your comment of March 10 says,
"work is still progressing to identify the correct place in the new structures of ICD-11," which implies that TAG Neurology has not yet reached consensus over its proposals for (I presume) the three ICD-10 legacy entities,
Postviral fatigue syndrome;
Benign myalgic encephalomyelitis; and
Chronic fatigue syndrome.
If TAG Neurology has still to reach consensus, could you please set out what are the implications for:
a) a release of TAG Neurology's proposals before the March 30 proposal deadline?
b) the inclusion of TAG Neurology's proposals in the projected April 4 frozen version for field testing?
If TAG Neurology's proposals were to be published at some point between now and April 4, by what date will stakeholder comments on TAG's proposals need to be submitted in order for comments to be taken into consideration for the final version of ICD-11, that is projected for release at some point in 2018?
There is no information on the Beta draft that states for how long the comment period will remain open to receive comments on proposals that have been submitted before the March 30 deadline. This is information of relevance to all stakeholder groups.
I make no apology for the length of this comment and trust that the lack of clarity over the past few weeks will now be addressed.
Stakeholders in these ICD-10 entities have now been subject to a four year period during which there has been no transparency of process - this serves no-one's interests.
[1] Summary Report, Third Meeting of the JLMMS Task Force Cologne, Germany, 11-14 April 2016 (p12 Exclusion Types)
http://www.who.int/entity/classifications/icd/revision/2016.04.11-14_iSummaryMeetingReportCologne.pdf
[2] Creed F, Gureje O. Emerging themes in the revision of the classification of somatoform disorders. Int Rev Psychiatry. 2012 Dec;24(6):556-67. doi: 10.3109/09540261.2012.741063. [PMID: 23244611]
[3] Gureje O, Reed GM. Bodily distress disorder in ICD-11: problems and prospects. World Psychiatry. 2016 Oct;15(3):291-292. doi: 10.1002/wps.20353. [PMID: 27717252]
Suzy Chapman 2017-Mar-11 - 13:25 UTC