Dx Revision Watch
Suzy Chapman Owner of Dx Revision Watch
- Messages
- 3,061
- Location
- UK
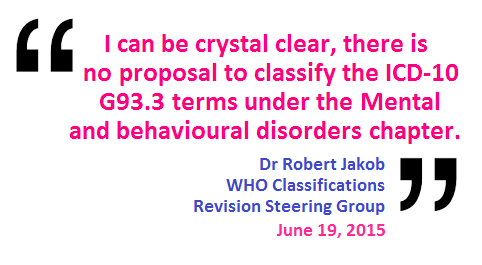
Dr Jakob is very familiar with the G93.3 terms, having been called upon over the years to issue clarifications in response to attempts by a WHO Collaborating Centre to blur the boundaries between a number of ICD-10 classifications, and in several reported instances, having swapped the G93.3 code for F48, because it suited their purpose to do so.
Dr Jakob knows very well that in ICD-10, there is a Fatigue syndrome inclusion under F48.0 Neurasthenia which has an Excludes for G93.3. He also knows that in ICD-10 under Malaise and fatigue there is also an Excludes for G93.3.
He knows there is no "chronic fatigue" category within ICD-10.
He knows that the three ICD-10 legacy terms for which information is being sought are:
Postviral fatigue syndrome
Benign myalgic encephalomyelitis
Chronic fatigue syndrome
He knows there is no Fatigue syndrome in ICD-11 Beta because the Neurasthenia category is retired for ICD-11. Bodily distress disorder subsumes and replaces most of ICD-10's somatoform disorders and Neurasthenia.
He knows that for ICD-11, Malaise and fatigue in the Symptoms, signs chapter has been changed to "Fatigue" and that there are no child categories sitting under "Fatigue."
But he appears to be having a lot of trouble articulating the names of the G93.3 legacy terms.
Whenever I write to ICD Revision or about ICD Revision, I am always precise. I always set out the three category terms that I am enquiring about because these are the "Concept Title" and "entity" terms, as classified within ICD-10:
Postviral fatigue syndrome
Benign myalgic encephalomyelitis
Chronic fatigue syndrome
But what do I get back from Dr Jakob, these days?
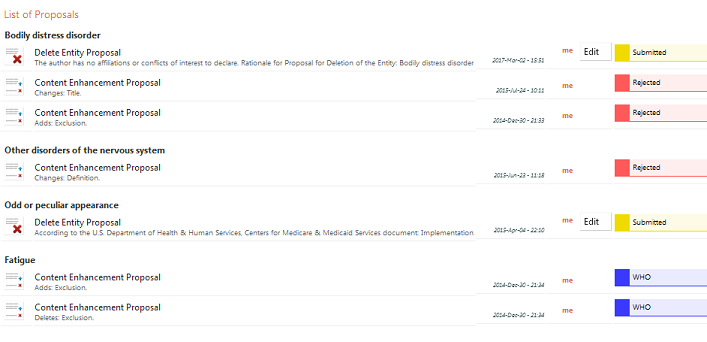
"Further to our earlier correspondence and phone calls, including contacts with other parties linked to chronic fatigue, I reiterate that WHO appreciates the work that you and others have put in to chronic fatigue. So far, you submitted 6 proposals linked to 3 entities on the proposal platform. All were submitted in time to be addressed for the field testing version that will be released on 4 of April."
And what is the response he gives to the Department of Health to inform Lord O'Shaughnessy's Written Response to the Countess of Mar:
"...The WHO has also confirmed that the proposal submitted for chronic fatigue is currently with the relevant groups of the organisation to consider the scientifically-based placement of this condition in the classification. This will be included in the next version of ICD-11 to be released on 4 April 2017 for field testing."
To reiterate: I have had no correspondence with ICD Revision in relation to "chronic fatigue". I have put in no work on "chronic fatigue" whether appreciated or not.
I have submitted no proposals for "chronic fatigue" which are currently with ICD Revision groups or work groups for their review and consideration.
Last edited: