MPP Layman's Interpretation: I looked at my previous post with MPP results and I am left scratching my head. The Methylation cycle derivates all look good. SAM, SAH, HS, and Methionine are all in range. The ratio of SAM to SAH is okay. The SAM + SAH does not seem to imply CBS upregulation.
Glutathione (reduced) Deficiency: I have to guess this is caused by low Cysteine. Cysteine is also a pre-cursor to Taurine. Is something getting stuck at Cystathionine or Homosysteine? Homocysteine is at the high end of the range, but still in range. Maybe HS, while still in range, is getting converted a little slow or being pushed to Methionine rather than down the Trans-Sulfuration Pathway? Strangely, Cysteine was in range on the SpectraCell Nutrient Panel. What should I believe? Maybe a trial of NAC supplementation?
B2 Deficiency: Per SpectraCell Micronutrient test and OAT, I am low in B2. B2 is needed to convert B6 to it's active P5P form. And B6 is needed by the Trans-Sulfuration Pathway.
B6 Deficiency: Per SpectraCell Micronutrient test and OAT, I am low in B6. B6 is needed to convert Homocysteine into Cystathionine, and then to Cysteine. Maybe my deficiency in the conversion process is due to low B6?
B9 Deficiency: Per SpectraCell Micronutrient test, OAT, and MPP, I am low in B9. Maybe high dose methylfolate, at 12.6 mg per day, is not the whole answer. Maybe I need to add in some Folinic Acid. My Folinic Acid (WB) in whole blood cells seem to be low per MPP.
Taurine Deficiency: There seems to be some kind of relationship between Taurine, Muscle Cramps, and muscle damage [Source]. It also seems that Taurine can help reduce the sympathetic nervous system response i.e. Fight or Flight response. I found an interesting research article on NCBI here that shows the benefits of Taurine on Chronic Bladder Pain and Pelvic Pain. I was diagnosed with Pelvic Pain Dysfunction on 5/2/2017 and confirmed by Physical Therapist on 5/9/2017, because my Pelvic Muscles are very tight like "guitar strings." My PT described the evil cycle of Pelvic Pain Dysfunction with respect to Sympathetic Nervous System Response. The Sympathetic Nervous System Response feeds the pain and the chronic pain feeds the Sympathetic Nervous System Response. Maybe lifting Taurine can break the evil CPPS cycle?
Cysteine Deficiency: It appears that Cysteine is used for a number of important functions in the body. 1) incorporation into amino acid sequences of proteins, where cysteine promotes protein structure by sulfhydryl bonding; 2) ratelimiting precursor for glutathione synthesis; 3) precursor for taurine (used in bile formation and nerve function); 4) source of sulfate for connective tissue synthesis; 5) source of pyruvate for energy or glucose production; and 6) neurotransmitter [Source]. Symptoms of cysteine deficiency include: apathy, loss of pigmentation in hair, edema, lethargy, liver damage, muscle loss, skin lesions, weakness, fat loss, and slowed growth in children [Source].
This post by Rich VK suggests a temporary Cysteine deficiency as methylation starts-up. I started my Intentional Methyation Protocol on 2/16/2017 and did the MPP blood draw 1 month later on 3/28/2017. Maybe at time of MPP blood draw my methylation cycle was starting-up and robbing the trans-sulfuration pathway of methionine; therefore, lowering cysteine. Will this lift with time? Should I assist the Trans-sulfuration pathway during this time with Taurine, NAC, and/or Glutathione?
What to do now?
There is a simple diagram in this article which shows Methylation cycle, Trans-Sulfuration Pathway and Cysteine products: Sulfate, Taurine, Glutathione, and metallothionein.
I found an old Methylation Pathways Panel that looks very similar to mine with an interpretation from Rich VK here. He suggests that the CBS pathway is going too slow and may need to supplement with extra B2 and B6. My SpectraCell and OAT both show B2 and B6 deficiencies. I have changed my B-Complex to sublingual and added in some extra B2 FMN sublingual. See post #13 and #16 for my notes on B2 FMN. Maybe adding in the sublingual B-Complex and FMN B2 is why some of my symptoms seem to be improving? I am almost 3 months into this more intentional Methylation Protocol; however, I still feel I'm in the tuning phase trying to find the correct balance of nutrient support. Will Cysteine, Taurine, and Glutathione start lifting soon per Rich VK's 3rd month clinical observations?
Here are quotes from the other thread for FreshVeggies MPP results:
Additional Links that may be helpful:
Part 1: The Most Important Blood Test That Is Rarely Ever Run!
Part 2: The Four Pathways of Homocysteine – Are One Or More of Your Pathways Blocked?
Part 3: (Homocysteine) The BHMT Pathway
Part 4: Homocysteine and the Transsulfuration Pathway
N-acetylcysteine in psychiatry: current therapeutic evidence and potential mechanisms of action - NCBI
Problems? I Have a NAC for That - Psychology Today
Glutathione: We Loves It (NAC and Autism) - Evolutionary Psychiatry
NAC Cysteine - Balancing Brain Chemistry
The Glutathione/Sulfation/Methylation Pathway - Autism Coach
Glutathione (reduced) Deficiency: I have to guess this is caused by low Cysteine. Cysteine is also a pre-cursor to Taurine. Is something getting stuck at Cystathionine or Homosysteine? Homocysteine is at the high end of the range, but still in range. Maybe HS, while still in range, is getting converted a little slow or being pushed to Methionine rather than down the Trans-Sulfuration Pathway? Strangely, Cysteine was in range on the SpectraCell Nutrient Panel. What should I believe? Maybe a trial of NAC supplementation?
B2 Deficiency: Per SpectraCell Micronutrient test and OAT, I am low in B2. B2 is needed to convert B6 to it's active P5P form. And B6 is needed by the Trans-Sulfuration Pathway.
B6 Deficiency: Per SpectraCell Micronutrient test and OAT, I am low in B6. B6 is needed to convert Homocysteine into Cystathionine, and then to Cysteine. Maybe my deficiency in the conversion process is due to low B6?
B9 Deficiency: Per SpectraCell Micronutrient test, OAT, and MPP, I am low in B9. Maybe high dose methylfolate, at 12.6 mg per day, is not the whole answer. Maybe I need to add in some Folinic Acid. My Folinic Acid (WB) in whole blood cells seem to be low per MPP.
Taurine Deficiency: There seems to be some kind of relationship between Taurine, Muscle Cramps, and muscle damage [Source]. It also seems that Taurine can help reduce the sympathetic nervous system response i.e. Fight or Flight response. I found an interesting research article on NCBI here that shows the benefits of Taurine on Chronic Bladder Pain and Pelvic Pain. I was diagnosed with Pelvic Pain Dysfunction on 5/2/2017 and confirmed by Physical Therapist on 5/9/2017, because my Pelvic Muscles are very tight like "guitar strings." My PT described the evil cycle of Pelvic Pain Dysfunction with respect to Sympathetic Nervous System Response. The Sympathetic Nervous System Response feeds the pain and the chronic pain feeds the Sympathetic Nervous System Response. Maybe lifting Taurine can break the evil CPPS cycle?
Cysteine Deficiency: It appears that Cysteine is used for a number of important functions in the body. 1) incorporation into amino acid sequences of proteins, where cysteine promotes protein structure by sulfhydryl bonding; 2) ratelimiting precursor for glutathione synthesis; 3) precursor for taurine (used in bile formation and nerve function); 4) source of sulfate for connective tissue synthesis; 5) source of pyruvate for energy or glucose production; and 6) neurotransmitter [Source]. Symptoms of cysteine deficiency include: apathy, loss of pigmentation in hair, edema, lethargy, liver damage, muscle loss, skin lesions, weakness, fat loss, and slowed growth in children [Source].
This post by Rich VK suggests a temporary Cysteine deficiency as methylation starts-up. I started my Intentional Methyation Protocol on 2/16/2017 and did the MPP blood draw 1 month later on 3/28/2017. Maybe at time of MPP blood draw my methylation cycle was starting-up and robbing the trans-sulfuration pathway of methionine; therefore, lowering cysteine. Will this lift with time? Should I assist the Trans-sulfuration pathway during this time with Taurine, NAC, and/or Glutathione?
When the methylation protocol is begun, the activity of the methionine synthase enzyme in the liver is increased by supplementing B12 and folate forms. This causes more of the homocysteine to be converted to methionine, so less is available to support synthesis of glutathione. One result of this is that the cystine level in the blood goes down, so that less of it is available to the brain.
Yes, ultimately the methylation protocol does increase glutathione. We have documented that with lab testing.
However, the very first thing that happens when B12 and folate are applied together, which is the real essence of this protocol, is that the activity of the methionine synthase enzyme is increased. This enzyme converts homocysteine to methionine. When that starts, there is initially less homocysteine available to enter the transsulfuration pathway, and that ends up lowering the production of cysteine and hence, glutathione.
Over time, the methylation cycle is able to fill by recycling homocysteine to methionine, and then there is more homocysteine available to enter the transsulfuration pathway.
In our clinical study, our first test point after starting the protocol was at three months, and at that point the glutathione level had increased significantly. But at early times, it makes sense that glutathione would initially drop, and that does seem to correspond to the increased excitotoxicity that many people report.
What to do now?
There is a simple diagram in this article which shows Methylation cycle, Trans-Sulfuration Pathway and Cysteine products: Sulfate, Taurine, Glutathione, and metallothionein.
I found an old Methylation Pathways Panel that looks very similar to mine with an interpretation from Rich VK here. He suggests that the CBS pathway is going too slow and may need to supplement with extra B2 and B6. My SpectraCell and OAT both show B2 and B6 deficiencies. I have changed my B-Complex to sublingual and added in some extra B2 FMN sublingual. See post #13 and #16 for my notes on B2 FMN. Maybe adding in the sublingual B-Complex and FMN B2 is why some of my symptoms seem to be improving? I am almost 3 months into this more intentional Methylation Protocol; however, I still feel I'm in the tuning phase trying to find the correct balance of nutrient support. Will Cysteine, Taurine, and Glutathione start lifting soon per Rich VK's 3rd month clinical observations?
Here are quotes from the other thread for FreshVeggies MPP results:
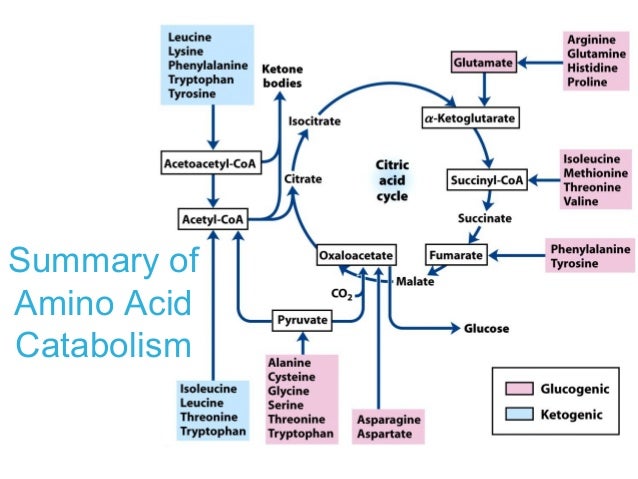
The CBS SNP does not seem to be impacting your methylation cycle. Your SAMe level is normal, and your SAH is high. Your glutathione is depleted. All of this suggests that you have low flow into your transsulfuration pathway, rather than high flow, as the CBS SNPs tend to give a person. My guess is that you are low in vitamin B6 and/or B2, so a B-complex should help you. You may also need some magnesium. I would suggest adding these to the simplified methylation protocol. I would not recommend lowering your protein intake. It is about the only fuel many PWCs can burn, becuase of a partial block early in the Krebs cycle, due to glutathione depletion, which you have. I haven't heard that Yucca causes leaky gut. I wonder if there is a reference for that.
The SNPs only give tendencies. They don't tell you what is actually happening in the person's biochemistry. FV's results on these two panels together are a good example of why I favor running the methylation pathways panel. She does have a heterozygous SNP on one of the CBS genes, but it is clear from her SAMe plus SAH concentrations that her methylation cycle has not been drained. The same appears to be true of yours.
The CBS enzyme requires activated B6 (P5P) for its operation. If B6 (or B2, needed to convert it to P5P) are low, this will inhibit the CBS reaction, and possibly also the CTH reaction (which also needs P5P), which is the other one in the transsulfuration pathway. If these are deficient, there will be low flow through transsulfuration, even if there are CBS SNPs.
It is necessary to have good flow down the transsulfuration pathway to make cysteine. About half the body's cysteine is normally made this way. Cysteine is usually the rate-limiting amino acid for making glutathione. So low flow into transsulfuration is consistent with inability to maintain a normal glutathione level.
Additional Links that may be helpful:
Part 1: The Most Important Blood Test That Is Rarely Ever Run!
Part 2: The Four Pathways of Homocysteine – Are One Or More of Your Pathways Blocked?
Part 3: (Homocysteine) The BHMT Pathway
Part 4: Homocysteine and the Transsulfuration Pathway
N-acetylcysteine in psychiatry: current therapeutic evidence and potential mechanisms of action - NCBI
Problems? I Have a NAC for That - Psychology Today
Glutathione: We Loves It (NAC and Autism) - Evolutionary Psychiatry
NAC Cysteine - Balancing Brain Chemistry
The Glutathione/Sulfation/Methylation Pathway - Autism Coach
Last edited: