Simon
Senior Member
- Messages
- 3,789
- Location
- Monmouth, UK
@Jonathan Edwards @taniaaust1 @Woolie @alex3619 continuing the discussion started here, as this thread seems more relevant
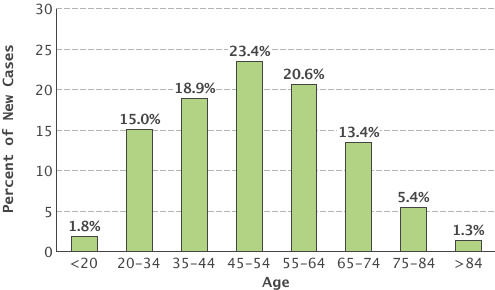
Some more about how this data was collected, as it's fascinating but far from bullletproof. It comses from the vast Norwegian national health database, looking at new 'cfs' cases diagnosed from 2008-2012
Even so, 5,800 new cases, of which 1,380 were in the 10-19 age group.
more later.
I know lots of stuff suggests the younger you are, the better your prognosis, and that could well be true. But there's another possiblility: it could be if you're younger, the onset of your CFS is more likely to be acute EBV. And it could be that EBV-onset has a slightly better prognosis.
That's a really interesting observation!
It ties in with the idea of an early 'mono/EBV' peak, and a separate, later adult peak, quite possibly with very different causes:
Two age peaks in the incidence of chronic fatigue syndrome/myalgic encephalomyelitis: a population-based registry study from Norway 2008¿20127
Figure One: twin age peaks:

(this image may be copyright: it's from the linked open source paper above, but please don't reproduce without linking to the original paper and explaining it may be copyright).
I haven't seen anything that says what proportion of adolescents with mecfs had it post mon/EBV, but get the impression it's most of them.
The incidence graph in brown and blue seems to me to tell us more than almost everything else we know about ME/CFS. Epidemiology generally doesn't lie and it forces constraints on any hypothesis right at the start.
My initial reactions are that:
1. There are obviously two diseases. This is not a wobble.
2. The first disease does NOT look like EBV, it starts too early.
3. The first disease does not fit either with the 'high achiever crash/yuppie flu' concept, which ought to be more 18-28.
4. The second disease is NOT a typical autoimmune disease because it tails off by 60. A purely B cell stochastic process should go on getting commoner with age until you start to exhaust the susceptible genetic pool (which happens for RA and breast cancer only around 85). The only autoimmune disease that has this sort of curve is lupus.
5. The first disease could be a T cell disease such as type I diabetes or an adolescent immune disease like anti-DEK+ve oligoarthritis (one of the common childhood arthropathies).
6. The early curves for boys and girls look more or less identical to what Esther Crawley reports, which gives reassurance that this is bona fide and not skewed by some local cultural factor.
7. This is why we need more population based studies! And what we need is to have a population for which curves can be constructed for known T and B cell diseases, EBV, reactive affective disorders (i.e. depression, phobias etc.) and anything else relevant.
Does the age curve not reflect wpmen caring for infeced schoolchildren?
It might be two diseases, I have favoured that idea for some time. However it could also be two pathways to the same end state, perhaps with two different risk factor profiles, including hormonal changes.
Some more about how this data was collected, as it's fascinating but far from bullletproof. It comses from the vast Norwegian national health database, looking at new 'cfs' cases diagnosed from 2008-2012
So note a) doesn't include primary care (maybe all cases get referred on too specialist centres? I don't know); b) a diagnosis is mandatory for doctors to get paid, they might not be thinking too hard about it, and different doctors may diagnose differently - there were no agreed case definitions used.For each hospitalization or outpatient visit, reporting of data to the NPR is mandatory and is linked to the reimbursement system...
Cases of CFS/ME were all in- and outpatients in Norwegian hospitals who were registered with the ICD-10 code G93.3 (‘postviral fatigue syndrome/benign myalgic encephalomyelitis’). Data from mental health care facilities were not included.
Even so, 5,800 new cases, of which 1,380 were in the 10-19 age group.
more later.

") and he is involved in the CFI Chronic Fatigue Initiative here in the US as well.
and he is involved in the CFI Chronic Fatigue Initiative here in the US as well.