
Dx Revision Watch
Suzy Chapman Owner of Dx Revision Watch
- Messages
- 3,061
- Location
- UK
There is already a thread on the monitoring of ICD-11 that I started a couple of years ago, but I think this merits a new thread. When I have located it, I will insert the link for the existing thread, for ease of reference.
19 February 2012
This is a longish post but it contains an important update on proposals for ICD-11 Chapter 5: Mental and behavioural disorders
Permission to republish, if published in full and with source and website attribution. A version of this report is published on Co-Cure Listserv and a version will be published on Dx Revision Watch later today.
In an interview with Tom Sullivan, last week, for Health Care Finance News, Christopher Chute, who chairs the ICD-11 Revision Steering Group, intimated a possible delay for completion of ICD-11 from 2015 to 2016. Nevertheless, an ICD-11 Beta drafting platform remains scheduled to launch in May, this year.
The Beta draft will take the form of a publicly viewable browser platform similar to the Alpha drafting platform that has been in the public domain since last May.
You can view the entry pages for the Alpha Drafting Browser here:
Foundation Component view:
http://apps.who.int/classifications/icd11/browse/f/en
Morbidity Linearization view:
http://apps.who.int/classifications/icd11/browse/l-m/en
A User Guide is here:
http://apps.who.int/classifications/icd11/browse/Help/en
The various ICD Revision Topic Advisory Groups (TAGs) are carrying out their work on a separate, more complex, multi-author drafting platform.
When the Beta drafting platform is launched, interested stakeholders will be invited to register for increased access for interacting with the drafting process by submitting comments and suggestions on the draft.
It is also possible to register for increased access to the Alpha drafting platform and to download PDFs of drafts for the "Print Versions for the ICD-11 Alpha Morbidity Linearization" for each chapter of ICD-11.
Caveats
I'm going to reiterate the ICD-11 Alpha Browser Caveats because it's important to understand that the ICD-11 Alpha draft is a work in progress:
The draft is updated on a (usually) daily basis; when you view the Alpha Browser, you are viewing a "snapshot" of how the publicly viewable draft stood at the end of the previous day; not all chapters are as advanced as others for organization and completion of content; the draft is incomplete and may contain errors and omissions; the codes and "sorting labels" assigned to ICD parent classes and child categories may change as work on the draft progresses and according to the reorganization of chapters; the Alpha draft has not yet been approved by the Topic Advisory Groups, Revision Steering Group or WHO and content in the draft may not progress to the Beta drafting stage.
We may have a clearer idea of what is being proposed when the Beta drafting platform is released, but at the moment, the Alpha lacks clarity; not all of the textual content has been generated and added to this section of the draft; not all of the 13 "Content Model" parameters display in the public version of the draft, and for those that do, not all have been populated with definitions and other textual content.
The two chapters of most relevance to us are Chapter 5: Mental and behavioural disorders and Chapter 6: Disorders of the nervous system (the Neurology chapter). (ICD-11 is dropping the use of Roman numerals.) I'm not going to discuss Chapter 6 in this post but I will do a follow up post for Chapter 6 in a few days, again there is a lack of clarity and requests for clarification from the chair TAG Neurology and the lead WHO Secretariat for TAG Neurology have met with no response.
ICD-10 Chapter 5 "Somatoform Disorders"
This is the section that corresponds with the current "Somatoform Disorders" section in DSM-IV.
You can compare the current DSM-IV "Somatoform Disorders" categories with the current ICD-10 "Somatoform Disorders" categories in this (simpified) table which lists only the category terms, not the criteria:
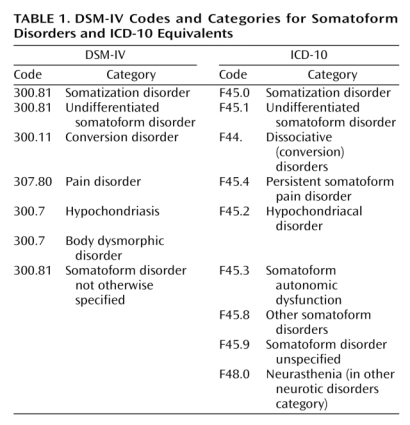
For those not aware of DSM-5 proposals: The DSM-5 "Somatic Symptom Disorders" Work Group proposes to rename its "Somatoform Disorders" section to "Somatic Symptom Disorders" and to roll a number of existing disorders within this section into a brand new category, "Complex Somatic Symptom Disorder" (which would include the previous diagnoses of somatization disorder [DSM IV code 300.81], undifferentiated somatoform disorder [DSM IV code 300.81], hypochondriasis [DSM IV code 300.7], as well as some presentations of pain disorder [DSM IV code 307]) and the more recently proposed, "Simple Somatic Symptom Disorder," which requires a somatic symptom duration of just one month, as opposed to six months to meet the CSSD criteria.
You can view the criteria for CSSD and SSSD as they stood last May, at the second public review and comment exercise, here on my site:
http://dxrevisionwatch.wordpress.com/dsm-5-proposals/dsm-5-proposals-sub-page-1/dsm-5-drafts-2/
Up until recently, the ICD-11 Alpha draft listings for the Chapter 5: Somatoform Disorders section were little changed from those in ICD-10, with the exception of what appears to be a new category called "05A08.06.01 Chronic pain disorder with somatic and psychological factors" which doesn't appear in ICD-10 Version: 2010 under F45.4.
(That might be problematic for Fibromyalgia patients.)
When I checked the Alpha Browser on 17 February, this section for "Somatoform Disorders" has been reorganized.
"Bodily Distress Disorders" to replace "Somatoform Disorders" category for ICD-11?
Please study this screenshot:
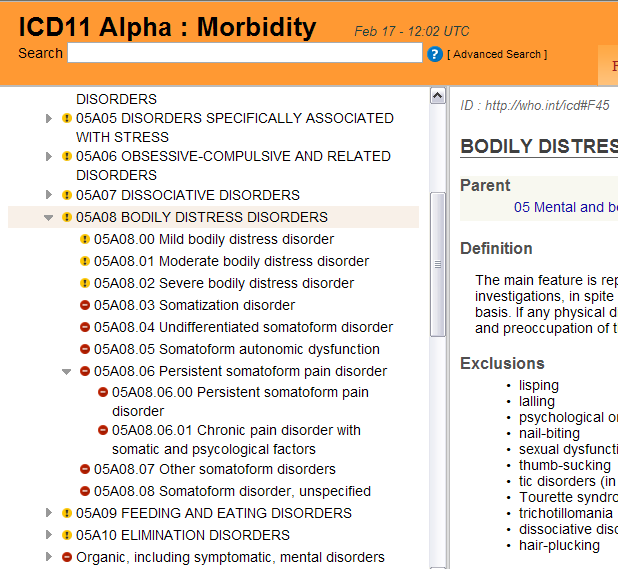
and this page on the Alpha Browser (click the little arrows to display the dropdown child categories):
http://apps.who.int/classifications/icd11/browse/l-m/en#/http://who.int/icd#F45
If you can't view the images that section looks like this:
05A08 BODILY DISTRESS DISORDERS
05A08.00 Mild bodily distress disorder
05A08.01 Moderate bodily distress disorder
05A08.02 Severe bodily distress disorder
05A08.03 Somatization disorder
05A08.04 Undifferentiated somatoform disorder
05A08.05 Somatoform autonomic dysfunction
05A08.06 Persistent somatoform pain disorder
05A08.06.00 Persistent somatoform pain disorder
05A08.06.01 Chronic pain disorder with somatic and psychological factors
05A08.07 Other somatoform disorders
05A08.08 Somatoform disorder, unspecified
Continued in next post
19 February 2012
This is a longish post but it contains an important update on proposals for ICD-11 Chapter 5: Mental and behavioural disorders
Permission to republish, if published in full and with source and website attribution. A version of this report is published on Co-Cure Listserv and a version will be published on Dx Revision Watch later today.
In an interview with Tom Sullivan, last week, for Health Care Finance News, Christopher Chute, who chairs the ICD-11 Revision Steering Group, intimated a possible delay for completion of ICD-11 from 2015 to 2016. Nevertheless, an ICD-11 Beta drafting platform remains scheduled to launch in May, this year.
The Beta draft will take the form of a publicly viewable browser platform similar to the Alpha drafting platform that has been in the public domain since last May.
You can view the entry pages for the Alpha Drafting Browser here:
Foundation Component view:
http://apps.who.int/classifications/icd11/browse/f/en
Morbidity Linearization view:
http://apps.who.int/classifications/icd11/browse/l-m/en
A User Guide is here:
http://apps.who.int/classifications/icd11/browse/Help/en
The various ICD Revision Topic Advisory Groups (TAGs) are carrying out their work on a separate, more complex, multi-author drafting platform.
When the Beta drafting platform is launched, interested stakeholders will be invited to register for increased access for interacting with the drafting process by submitting comments and suggestions on the draft.
It is also possible to register for increased access to the Alpha drafting platform and to download PDFs of drafts for the "Print Versions for the ICD-11 Alpha Morbidity Linearization" for each chapter of ICD-11.
Caveats
I'm going to reiterate the ICD-11 Alpha Browser Caveats because it's important to understand that the ICD-11 Alpha draft is a work in progress:
The draft is updated on a (usually) daily basis; when you view the Alpha Browser, you are viewing a "snapshot" of how the publicly viewable draft stood at the end of the previous day; not all chapters are as advanced as others for organization and completion of content; the draft is incomplete and may contain errors and omissions; the codes and "sorting labels" assigned to ICD parent classes and child categories may change as work on the draft progresses and according to the reorganization of chapters; the Alpha draft has not yet been approved by the Topic Advisory Groups, Revision Steering Group or WHO and content in the draft may not progress to the Beta drafting stage.
We may have a clearer idea of what is being proposed when the Beta drafting platform is released, but at the moment, the Alpha lacks clarity; not all of the textual content has been generated and added to this section of the draft; not all of the 13 "Content Model" parameters display in the public version of the draft, and for those that do, not all have been populated with definitions and other textual content.
The two chapters of most relevance to us are Chapter 5: Mental and behavioural disorders and Chapter 6: Disorders of the nervous system (the Neurology chapter). (ICD-11 is dropping the use of Roman numerals.) I'm not going to discuss Chapter 6 in this post but I will do a follow up post for Chapter 6 in a few days, again there is a lack of clarity and requests for clarification from the chair TAG Neurology and the lead WHO Secretariat for TAG Neurology have met with no response.
ICD-10 Chapter 5 "Somatoform Disorders"
This is the section that corresponds with the current "Somatoform Disorders" section in DSM-IV.
You can compare the current DSM-IV "Somatoform Disorders" categories with the current ICD-10 "Somatoform Disorders" categories in this (simpified) table which lists only the category terms, not the criteria:
For those not aware of DSM-5 proposals: The DSM-5 "Somatic Symptom Disorders" Work Group proposes to rename its "Somatoform Disorders" section to "Somatic Symptom Disorders" and to roll a number of existing disorders within this section into a brand new category, "Complex Somatic Symptom Disorder" (which would include the previous diagnoses of somatization disorder [DSM IV code 300.81], undifferentiated somatoform disorder [DSM IV code 300.81], hypochondriasis [DSM IV code 300.7], as well as some presentations of pain disorder [DSM IV code 307]) and the more recently proposed, "Simple Somatic Symptom Disorder," which requires a somatic symptom duration of just one month, as opposed to six months to meet the CSSD criteria.
You can view the criteria for CSSD and SSSD as they stood last May, at the second public review and comment exercise, here on my site:
http://dxrevisionwatch.wordpress.com/dsm-5-proposals/dsm-5-proposals-sub-page-1/dsm-5-drafts-2/
Up until recently, the ICD-11 Alpha draft listings for the Chapter 5: Somatoform Disorders section were little changed from those in ICD-10, with the exception of what appears to be a new category called "05A08.06.01 Chronic pain disorder with somatic and psychological factors" which doesn't appear in ICD-10 Version: 2010 under F45.4.
(That might be problematic for Fibromyalgia patients.)
When I checked the Alpha Browser on 17 February, this section for "Somatoform Disorders" has been reorganized.
"Bodily Distress Disorders" to replace "Somatoform Disorders" category for ICD-11?
Please study this screenshot:
and this page on the Alpha Browser (click the little arrows to display the dropdown child categories):
http://apps.who.int/classifications/icd11/browse/l-m/en#/http://who.int/icd#F45
If you can't view the images that section looks like this:
05A08 BODILY DISTRESS DISORDERS
05A08.00 Mild bodily distress disorder
05A08.01 Moderate bodily distress disorder
05A08.02 Severe bodily distress disorder
05A08.03 Somatization disorder
05A08.04 Undifferentiated somatoform disorder
05A08.05 Somatoform autonomic dysfunction
05A08.06 Persistent somatoform pain disorder
05A08.06.00 Persistent somatoform pain disorder
05A08.06.01 Chronic pain disorder with somatic and psychological factors
05A08.07 Other somatoform disorders
05A08.08 Somatoform disorder, unspecified
Continued in next post
