
-

Welcome to Phoenix Rising!
Created in 2008, Phoenix Rising is the largest and oldest forum dedicated to furthering the understanding of, and finding treatments for, complex chronic illnesses such as chronic fatigue syndrome (ME/CFS), fibromyalgia, long COVID, postural orthostatic tachycardia syndrome (POTS), mast cell activation syndrome (MCAS), and allied diseases.
To become a member, simply click the Register button at the top right.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Action for M.E. (2003). Membership survey ‘your experiences’ questionnaire
- Thread starter Dolphin
- Start date
Example 1 of Peter White quoting this survey:
In:
(other references to harm in paper:
In:
Clark, L. V. & White, P. D. The role of deconditioning and therapeutic exercise in chronic fatigue syndrome (CFS). Journal of Mental Health, 2005, 14(3), 237-252.
Does therapeutic exercise cause harm?
There is a discrepancy between reports of self-help group members and published evidence from trials in this matter. Fifty per cent of 2,338 members of the largest self-help group in the UK, Action for M.E., reported that they felt worse after exercise therapy, whereas the trial evidence suggests minimal or no risk with these treatments (Action for ME, 2001). However, a further survey by Action for M.E. of their members in 2003 (Action for ME, 2003) suggests that reports of deterioration following therapy were related to either poorly administered treatment or lack of appropriate professional supervision, rather than GET itself. Properly administered GET requires an appropriately qualified and trained professional, such as a physiotherapist, mutually agreeing with the patient and adjusting the programme depending on their response. The recent systematic review by Edmonds et al. (2004) concludes that, on average, there is no evidence that GET may worsen outcomes in patients with CFS.
(other references to harm in paper:
Summary:
[..]
There is little evidence of harm in published trials using GET that is properly supervised by an appropriate professional and mutually agreed with the patient.
Abstract:
[..]
Patient education is necessary to inform patients of the positive benefit/risk ratio in order to improve acceptance and adherence.
Example #2 of Peter White quoting this survey:
In
In
Protocol for the PACE trial: a randomised controlled trial of adaptive pacing, cognitive behaviour therapy, and graded exercise, as supplements to standardised specialist medical care versus standardised specialist medical care alone for patients with the chronic fatigue syndrome/myalgic encephalomyelitis or encephalopathy.
White PD, Sharpe MC, Chalder T, DeCesare JC, Walwyn R; PACE trial group.
BMC Neurol. 2007 Mar 8;7:6.
Risks and benefits
There is a discrepancy between surveys of CFS/ME patient group members and published evidence from trials. Some CFS/ME charity members have reported that they feel worse after exercise therapy, and to a lesser extent CBT [13,14], whereas the trial evidence suggests minimal or no risk with these treatments. A further survey by Action for M.E. of their members suggests that reports of deterioration with therapy are related to either poorly administered treatment or lack of appropriate professional supervision [15]. The individual treatment programmes used in PACE will minimise this risk by being mutually agreed between participant and therapist, carefully monitored and flexibly implemented. We will also carefully monitor all participants for any adverse effects of the treatments, and will undertake a detailed assessment, at home if necessary, of any participant who reports deterioration or who withdraws from treatment, following which they will be offered appropriate help.
13. Action for M.E.: Severely neglected ME in the UK. London, Action for M.E.; 2001.
14. Cooper L. London: Action for M.E. and the ME association: Report on survey of members of local ME groups. 2000.
15. Action for M.E.: Membership Survey 'your experiences' questionnaire. Wells , Action for M.E; 2003.
Example #3 of Peter White quoting this survey:
In:
In:
J Rehabil Med. 2008 Nov;40(10):882-3; author reply 883-5. doi: 10.2340/16501977-0261.
Chronic fatigue syndrome.
Clark LV, White PD.
Sir,
We read with interest the special report by Nijs et al. (1), entitled “Chronic fatigue syndrome: an approach combining self-management with graded exercise to avoid exacerbations”. The paper proposes to provide an integrated model for graded exercise therapy (GET) in patients with chronic fatigue syndrome (CFS).
The authors state that current GET programmes for people with CFS exacerbate symptoms. This is a familiar and mistaken criticism of GET, often quoted from the 2001 Action for myaligic encephalomyelitis (ME) (AfME) survey, which reported that 50% of patients with CFS/ME who received graded exercise felt worse (2). A follow-up survey reported that, in many cases, exercise was being undertaken independently, without the supervision of a therapist trained to deliver GET to patients with CFS (3). In other words, it was not GET.
<snip>
References
1. Nijs J, Paul L, Wallman K. Special report. Chronic fatigue syndrome: an approach to combining self-management with graded exercise to avoid exacerbations. J Rehabil Med 2008; 40; 241–247.
2. Action for ME (AfME). Severely neglected ME in the UK. London: Action for ME; 2001. Available from: http://www.afme.org.uk/res/
img/resources/Severely%20Neglected.pdf [accessed 2008 April30].
3. Action for ME (AfME). Membership survey. Learning from experience. London: Action for ME; 2003. Available from: http://
www.afme.org.uk/res/img/resources/IA%2045%20pages%204-5%20_research%20section.pdf [accessed 2008 April 30].
Example #4 of Peter White quoting this survey:
(see second paragraph)
(see second paragraph)
J Rehabil Med. 2010 Feb;42(2):184 -5
Clark LV, White PD.
Sir,
The UK National Institute for Clinical Excellence (NICE) guidelines on the management of CFS/ME recommends that we should “offer cognitive behavioural therapy (CBT) and/or GET to people with mild or moderate CFS/ME, and provide them for those who choose them, because these are the interventions for which there is the clearest research evidence of benefit” (13). The full guidelines go on to state that “unsuccessful general exercise programmes, perhaps undertaken independently by the patient, or under brief advice from professionals Letters to the Editor 185 not adequately trained in the use of GET, are often begun at a high, unachievable level, with an inappropriately rapid rate of progression, or without adequate professional supervision or support. An unstructured and poorly monitored or progressed exercise programme can cause significant symptom exacerbation, and can arguably make CFS/ME worse” (13).
This view agrees with the one patient charity survey that attempted to explain the discrepancy in adverse effects of GET between published research and patient charity member surveys. “When those who had had GET in the last 3 years were examined in more depth, a high proportion had never in fact [received] GET as reported in research studies.... This appears to show that outside the major ME centres, who does it and to what standard is a lottery. Suggesting that the issue may not be the value of GET, but what type and the quality of the therapist. This would certainly support the evidence given to the Chief Medical Officer’s (CMO) Report, and, if true, could explain why harm is not found through research trials (conducted in the best centres), but is found through surveys of people’s experiences – few having had access to the best centres” (14). Any effective medical intervention that is improperly given may cause harm. We believe the issue here is not the safety of GET, but its proper implementation and availability. The NICE guidelines provide an excellent description of how to carry out GET safely and effectively (13).
As to our own pilot study, suggesting that acute aerobic exercise (not GET) may be associated with elevated concentrations of certain cytokines (10), we are currently undertaking a proof of principle study. Finally, the PACE trial (www.pacetrial.org) is the largest ever trial of GET for patients with CFS/ME, and adaptive pacing therapy is one of the comparison treatments (15). We will soon have even more data that tests both the efficacy and safety of GET when compared with other non-pharmacological interventions; the main results are expected in 2010.
Lucy V. Clark, PhD* and Peter D. White, MD From the Barts and the London School of Medicine & Dentistry, Queen Mary University of London, Wolfson Institute of Preventive Medicine, PACE Trial Office, Suite 3.1, Dominion House, 59, Bartholomew Close, London, EC1A 7ED, UK. *E-mail: l.clark@qmul.ac.uk
Example #5 of Peter White quoting this survey:
PD White didn't write this extract - this was written by ScotME:
PACE trial – back it, say the organisers. Dr. Peter White, Professor Michael Sharpe, and Professor Trudie Chalder. ME Essential, the magazine of The ME Association, Issue 92, October 2004, page 9.
Also a letter from the CMO!
PD White didn't write this extract - this was written by ScotME:
1) Inappropriate Application of CBT/GE It should not simply be assumed that any negative effects reported by patients following behavioural interventions such as exercise are due to inappropriate application. Despite a lack of evidence this is, however, a fairly common perspective.
• For example: “… reported negative effects were probably due to either inappropriate advice on how to do graded exercise therapy (such as a doctor telling a patient to join a gym) or to patients trying this approach unsupervised by the appropriate professional.”10 The authors refer to a survey by Action for ME in support of this contention.11 However, the published findings from this survey provide no evidence whatsoever regarding what might account for the negative impact reported. 12
• This is not the only example of this unfounded assumption. A letter written on behalf of the Chief Medical Officer (England and Wales) repeats the above quote almost verbatim, including reference to the Action for ME survey.13
References:
10 PACE trial – back it, say the organisers. Dr. Peter White, Professor Michael Sharpe, and Professor Trudie Chalder. ME Essential, the magazine of The ME Association, Issue 92, October 2004, page 9.
11 Action for ME Membership Survey ‘your experiences’ questionnaire. Wells, Action for ME, 2003.
12 Learning from experience. InterAction, Issue 45, August 2003, pages 4-5. The article states that 40% of those who had tried GET “had not had professional guidance or support” [page 4], but does not provide information as to whether or not this group were more - or indeed less - likely to report a negative impact.
13 Sent in reply to correspondence from Doris Jones concerning the MRC-funded PACE [Pacing, graded Activity, and Cognitive behavioural therapy: a randomised Evaluation] trial. Copy posted on CO-CURE@LISTSDERVE.NODAK.EDU May19th 2005].
Example #6 of Peter White quoting this survey:
In:
In:
http://www.pacetrial.org/docs/get-therapist-manual.pdf
Manual For Therapists
GRADED EXERCISE THERAPY FOR CFS/ME
Bavinton J, Darbishire L, White PD
On behalf of the PACE trial management group
ADVERSE EFFECTS OF GRADED EXERCISE THERAPY (GET)
Surveys by patient groups of their members have suggested that GET may be harmful to
some people with CFS/ME.26-28 It is now believed this finding was due to inappropriately
planned or progressed exercise programmes, possibly undertaken independently or
under supervision from a person without appropriate experience.28
28. Action for M.E. Membership Survey 'your experiences' questionnaire. Wells: Action for M.E., 2003.
Example #7 of Peter White quoting this survey:
Chronic fatigue syndrome or myalgic encephalomyelitis.
White P, Murphy M, Moss J, Armstrong G, Spencer P.
BMJ. 2007 Sep 1;335(7617):411-2. No abstract available.
PMID: 17762005 [PubMed - indexed for MEDLINE]
NICE guidelines pave the way forward for patients and doctors
[..]
Will the guidelines be useful and can they be implemented? The answers are yes and why not? The guidelines may seem too obvious to be useful, but this view underestimates the previous disagreement about how to help patients. A survey conducted by a national patient charity reported that half of patients found graded exercise therapy harmful,8 although a later survey showed that this was related to inappropriate advice or lack of therapeutic support.9
8. Action for ME. Severely neglected: ME in the UK, membership survey. 2001. www.afme.org.uk/res/img/resources/Severely%20Neglected.pdf.
9. Action for ME. All about ME: an introduction. 2004. www.afme.org.uk/res/img/resources/All%20about%20ME.pdf.
(9 presumably relates to the results in 2003)
From Full NICE guidelines - I'm not sure who made this point at the moment:
3.2 Summary of submissions by stakeholder organisations
3.2.1 Patient responses/experiences to management interventions for CFS/ME
3.2.1.1 Cognitive behavioural therapy (CBT)/modified CBT
• ‘13% were made worse by CBT, 32% were not helped at all, 37% were helped a little and 18% were helped a lot.’ (Report on Survey of Members of Local ME Groups, Cooper 2000)
• Mixed results for CBT depending on practitioner. Issues repeatedly cropped up about language and relationships indicating the problem may not be CBT but poorly practised CBT. (Action for ME, Members Survey, 2003)
• 7% found CBT helpful, 93% found CBT unhelpful. (25% ME Group, Analysis Report, 2004)
Bob
Senior Member
- Messages
- 16,455
- Location
- England (south coast)
That's an interesting graph. Where did you get the graph from, Dolphin?
That's an interesting graph. What did you get the graph from, Dolphin?
See attachment in top post.
Simon
Senior Member
- Messages
- 3,789
- Location
- Monmouth, UK
I thought I would upload this survey. Peter White often quotes this small survey and I think it is useful for people to be familiar with it.
Here's the main quantitative data on GET from the survey that I recall.
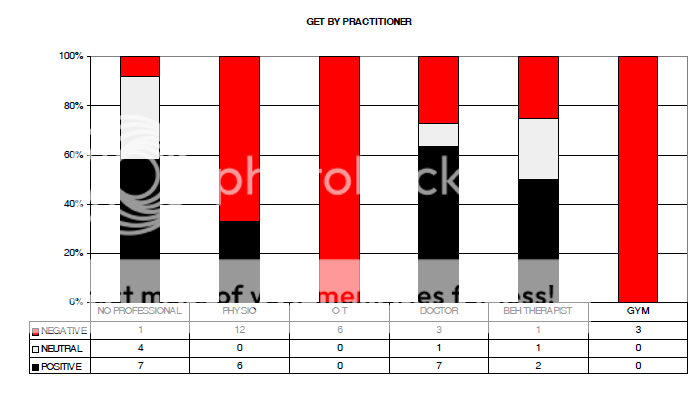
- Astonishing: you can't conclude anything at all from a sample of 42
- Comparing negative outcomes vs postivie/neutral, looking at the Behavioural Therapist results - presumably bona fide trained for such interventions - with gym gives a p value of 0.42, where p=0.05 is significant (Fisher's exact test)
- In any case, the best results came from using no professional (ranking from worst harm to least: OT = Gym < Physio < Therapist = GP < No Professional)
- So not only are the results statistically meaningless, the non-significant results indicate the results are worse with health professionals (Though amazingly the gym approach is bad too).
Bob
Senior Member
- Messages
- 16,455
- Location
- England (south coast)
Clearly AfME failed to refer to this graph when they wrote their published GET paper in which they heavily push the theory that any bad experiences in relation to GET are caused by badly trained therapists. Considering this data, I think their published GET paper undermines their members, and does us all a grave disservice. Instead of objectively assessing their own research results, they appear to have deferred to the psych-lobby, yet again. I'm really annoyed about this important omission from their research study. I wish I'd seen this data earlier. I didn't know it existed.
AfME always seem completely out of their depth in terms of interpreting research, or research proposals. Either that or consciously in collusion.
As Simon says, we can't tell much from this data, but it could have pointed them towards further research. Instead they've completely ignored it, and have almost concluded the opposite of what the data shows, but without any further evidence.
AfME always seem completely out of their depth in terms of interpreting research, or research proposals. Either that or consciously in collusion.
As Simon says, we can't tell much from this data, but it could have pointed them towards further research. Instead they've completely ignored it, and have almost concluded the opposite of what the data shows, but without any further evidence.