Mary Schweitzer Co-Cure post: ACT: ICD-9-CM and ICD-10-CM
----- Original Message -----
Sent: Monday, September 19, 2011 11:10 PM
Subject: [CO-CURE] ACT: ICD-9-CM and ICD-10-CM
There has been a lot of smoke around this subject lately, so since I've spent years on the subject and testified to CFSAC about it, I thought I should share what I know, and what I believe. (Besides, I don't want to have to write any more emails about it!)
The World Health Organization (WHO) puts out what is called the "International Classification of Disease," so that nations keep comparable statistics on diseases. About once a decade they revised it, until ICD-10, which took 15 years, and now ICD-11 has already taken more than 20.
Most nations just use the version published by WHO - and that includes the UK. A few nations (Canada, Australia, Germany, the U.S.) publish their own clinical manual. The rules they have agreed to as signatory nations is that it is okay to add a disease not in WHO's version, and they may subtract a disease that WHO includes but is not diagnosed in that country. They are NOT supposed to MOVE a disease into a different chapter altogether, because that would defeat the purpose of having international codes in the first place. The US versions are called ICD-9-CM and will be called ICD-10-CM.
There are two versions - the "tabular" version, which is organized by category, and the "index," which provides an alphabetized listing of specific medical conditions and directs you to the correct category. The tabular version is smaller, but the index version is just as authoritative.
For reasons that I cannot fathom, WHO only has the tabular version on Internet. But I have on my hard drive photocopied copies of the page in the printed index to ICD-10 that relates to CFS. "Syndrome, Fatigue, Chronic" goes in G93.3.
In 1969, WHO placed M.E. In the neurology chapter, giving it the code 323.9. They gave it the formal name it was first blessed with in the mid-1950s, "benign Myalgic Encephalomyelitis," because it didn't have a high mortality rate. However, The late Melvin Ramsay and other British experts immediately discarded the word "benign," because, as Ramsay put it, there was nothing "benign" about this disease! Why WHO keeps that word is beyond me, but the point is that M.E. had the code 323.9 under neurological conditions from 1969 on.
In 1988, a new name and definition was introduced to the world. The name was Chronic Fatigue Syndrome, and the definition is known as Holmes 1988 for the CDC epidemiologist who ran an earlier meeting to rename "Chronic Epstein-Barr." NOTHING, not even a footnote, in the Holmes 1988 article mentions M.E. or its American version, epidemic neuromyesthenia. But that same year the late Stephen Straus of NIAID at NIH published an article tying CFS to epidemic neuromyesthenia - and also to "mental health problems," citing two articles published in the early 1970s in the BMJ insisting that M.E. was really mass hysteria because the outbreaks occurred among female students and nurses living in residential dormitories. Soon British psychiatrist Simon Wessely had switched that to "neurasthenia" (citing a text written in 1869 - can you imagine the type of medical information available in 1869? The recommended action for a bullet in the leg was to saw the thing off.). Straus, Wessely, psychiatrist Peter White, and CDC's head of CFS, Bill Reeves, all juxtaposed the insistence that this disease was psychogenic with statements about it mainly impacting women - they even showed a slide of a woman in Edwardian dress lying back on a fainting couch. The American version did not use neurasthenia (which is not in DSM-IV), substituting instead "stress" - at first yuppie stress caused by "trying to have it all," later, an inability to handle "stress" caused by childhood traumas.
Chronic Fatigue Syndrome never made it into WHO's ICD-9 because by 1988, WHO was busy working on ICD-10, which was published a couple of years afterwards. So the US had carte blanche to put it where they wanted to. Since CDC liked to diagnose it by beginning with "chronic fatigue" and narrowing that down to "chronic fatigue syndrome," CFS was placed in the category "vague signs and symptoms," at 780.71.
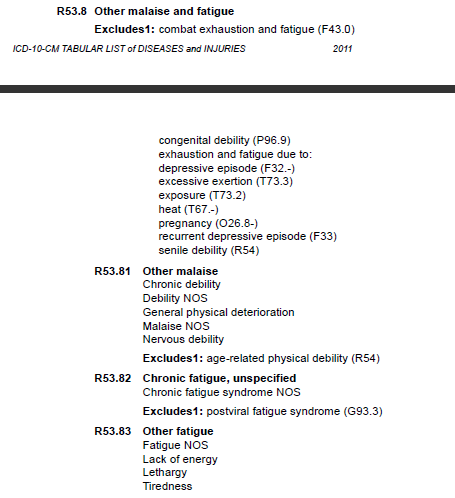
Those who have complained that CFS is treated like a "garbage diagnosis" - what's left over after everything else has been ruled out - can point to that designation as the reason. That is the chapter where you PUT a garbage diagnosis - and it would remain a "garbage diagnosis" in ICD-10-CM version if it was coded in chapter "R" at R53.82.
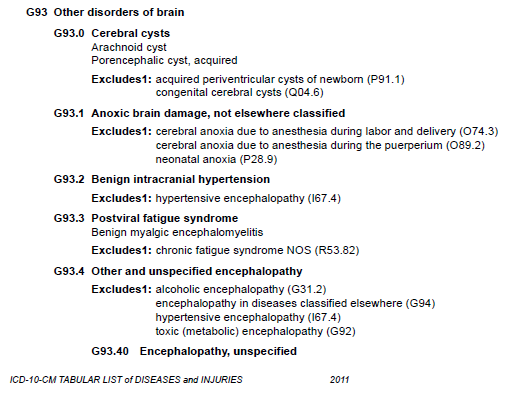
When WHO got around to coding CFS, it went into the same category as M.E. and a diagnosis not given that frequently any more, PVFS, or post-viral fatigue syndrome. That does not mean they are the same thing. It does mean that WHO considers them similar, and it also means that WHO decided CFS belonged in neurology, not "vague signs and symptoms."
British psychiatrists have tried to use "neurasthenia" (a nervous condition, the vapors, a nervous breakdown) instead of M.E., but they have been scolded by Parliament for doing so because it violates ICD-10. So the Peter White/Simon Wessely/Michael Sharpe crowd created the designation "fatigue syndrome," which IS coded to F48.0, or neurasthenia.
Trust me, this game is full of land mines.
ICD-10 was out and in use early in the 1990s. Canada adopted it soon after the millennium change, but where CFS was only in the index of ICD-10, Canada's version, ICD-10-CA, placed it in the tabular version at G93.3. Since some Canadian doctors diagnosed M.E. and others diagnosed CFS, the National M.E./FMS Society of Canada brought together an international committee of clinicians to create a CONSENSUS criteria, which was adopted by Canada in 2003. The document ran 100 published pages with a huge bibliography in the Journal of CFS, but Bruce Carruthers and Marjorie van de Sande wrote a summary, which we all know (and love) as that marvelous multicolored pamphlet that has been handed out all over the world, made available to all by the Canadian ME/FMS Society (with thanks to Lydia Neilson).
If you liked the Canadian Consensus Criteria, you should be pleased with the designation of CFS in G93.3 with M.E., because that is why it exists.
ICD-10 has been out in the world for twenty years now, and WHO is working on ICD-11. If it were up to me, we would, frankly, just skip ICD-10-CM altogether and wait a couple more years and then adopt ICD-11-CM, but we're not going to do that.
So, what are the choices for ICD-10-CM?
1. Reeves wanted it coded at R53.82 - that is, in the chapter on vague signs and symptoms, the garbage diagnosis chapter. WE WOULD BE THE ONLY NATION IN THE WORLD TO DO SO.
2. CFSAC has twice recommended we follow Canada's lead and put CFS in G93.3 with M.E. and PVFS. I think this is the simple and obvious solution - particularly since it is probable WHO will continue to code CFS and M.E. together in ICD-11.
3. I have heard of a compromise where CFS would be placed in neurology (thereby fulfilling the requirement that it remain in the same chapter), but place it in a different location in G. I disagree with this for the simple reason that we have NEVER fared well when CDC went against the rest of the world where our disease is concerned.
Back in the 1950s, when the rest of the world was diagnosing M.E., the U.S. went its own way with the name epidemic neuromyesthenia. That hurt us in the 1980s. Had the North Tahoe and Lyndonville outbreaks occurred in the UK, the patients would have been diagnosed with M.E. But M.E. was unknown in the US, and very few clinicians still alive used epidemic neuromyesthenia (plus the word "epidemic" gave CDC hives).
I vividly recall years when NCHS at CDC pulled M.E. from ICD-9-CM altogether. Because of that, most computerized coding systems (which is what everyone uses) do not even include 323.9 - and that can make it hard to get reimbursed for an M.E. diagnosis. I don't want to see G93.3 mysteriously disappear in the same fashion.
So - I think the U.S. should quit playing the Lone Ranger here, and support M.E. by supporting the designation of G93.3 for CFS. We can distribute both the 2003 Canadian consensus criteria and the new definition of M.E. that was published with an October 2011 date in the "Journal of Internal Medicine."
I have attended almost every CFSCC and CFSAC meeting since 1996 - sometimes in a wheelchair, but I was always there. I think our best argument for legitimizing M.E. is to point to it in ICD-10 and ICD-10-CA (Canada's version - Germany followed Canada, but Australia followed the UK. NOBODY followed the CDC.)
Mostly, however, I have enormous respect for our pragmatic, intelligent neighbors to the North. If Canada put CFS in G93.3, that's good enough for me.
Mary Schweitzer
Patient, advocate, author
---------------------------------------------
Send posts to
CO-CURE@listserv.nodak.edu
Unsubscribe at
http://www.co-cure.org/unsub.htm
Too much mail? Try a digest version. See
http://www.co-cure.org/digest.htm
---------------------------------------------
Co-Cure's purpose is to provide information from across the spectrum of
opinion concerning medical, research and political aspects of ME/CFS and/or
FMS. We take no position on the validity of any specific scientific or
political opinion expressed in Co-Cure posts, and we urge readers to
research the various opinions available before assuming any one
interpretation is definitive. The Co-Cure website <www.co-cure.org> has a
link to our complete archive of posts as well as articles of central
importance to the issues of our community.
---------------------------------------------