

Dx Revision Watch
Suzy Chapman Owner of Dx Revision Watch
- Messages
- 3,061
- Location
- UK
Screenshots from ICD-11 collaborative drafting platform (the iCAT)
Extracts from my Dx Revision Watch site June 2010 report:
PVFS, ME, CFS: the ICD-11 Alpha Draft and iCAT Collaborative Authoring Platform: http://wp.me/pKrrB-KK
For full notes that accompany these images, please see the report on my site.
The information in this post relates solely to proposals for ICD-11. It does not apply to ICD-10-CM, the forthcoming US “Clinical Modification” of ICD-10.
There are ICD-10 clinical modifications for ICD-10-AM [Australia], ICD-10-CA [Canada], ICD-10-GM [Germany], ICD-10-TM [Thailand] and ICD-10-CM [United States]. These ICD-10 modifications differ in their number of codes, chapters, and subcategories. Specific conditions are present in some but not all of the modifications.
The most recent release of proposals for ICD-10-CM (release for 2011), both the Index and Tabular List can be downloaded from the CDC site here: http://www.cdc.gov/nchs/icd/icd10cm.htm
ICD-11 screenshots from the iCAT drafting platform
The iCAT drafting platform was taken out of the public domain in November. The platform may be available again, in May, if the Beta Draft is ready by then. ICD Revision has been discussing the pros and cons of postponing the Beta until later this year, or possibly even next year.
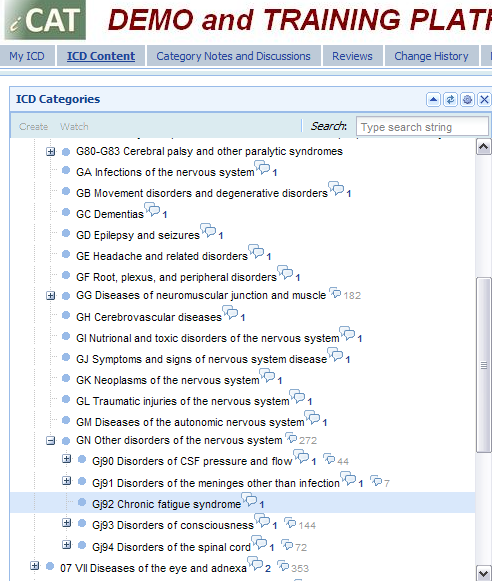
Chapter 6 Diseases of the nervous system
Note that existing ICD-10 codings between G83.9 and G99.8 are being reorganised and have been assigned the labels GA thru GN (some of which are parent categories with child and grandchildren categories).
GN Other disorders of the nervous system is a parent to category Gj92 Chronic fatigue syndrome
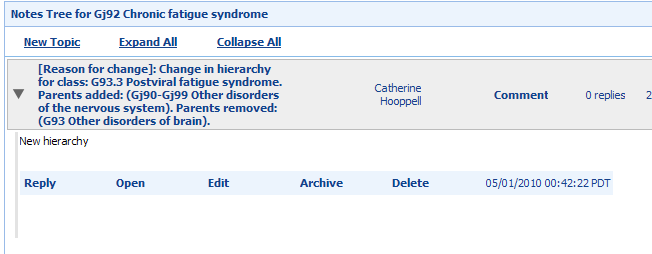
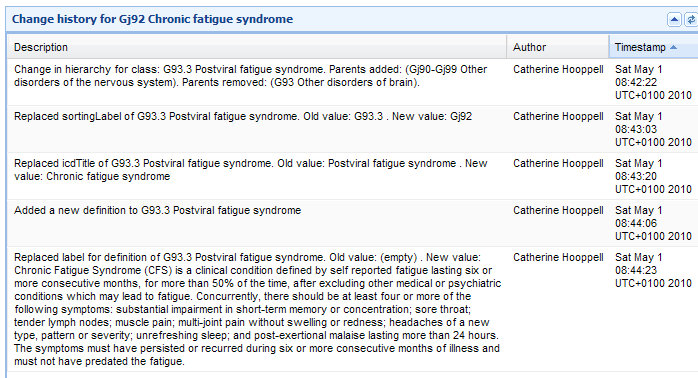
This iCAT Discussion Note for "Gj92 Chronic fatigue syndrome" records a Change in hierarchy for class: G93.3 Postviral fatigue syndrome because its parent category (G93 Other disorders of brain) is proposed to be removed.
Note that the removal of the parent G93 Other disorders of brain will affect many other categories that were also classified under G93 in ICD-10, not just G93.3.
Note that many categories in the G codes are undergoing reorganisation within Chapter 6 and have been assigned "Sorting labels". It is not known, at this stage, whether PVFS, CFS and ME will be reassigned the G93.3 code because of the reorganisation that is being undertaken within Chapter 6 and because of the removal of the parent term G93.
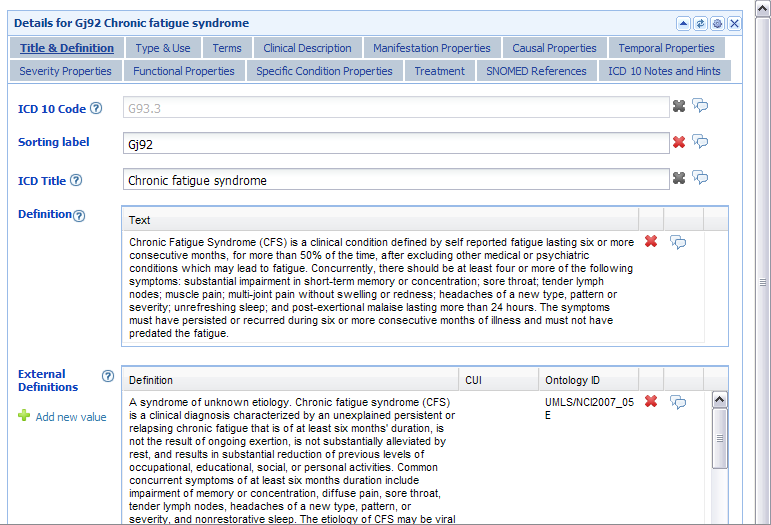
Note that three External Definitions (which aren't all visible in the screenshot, below, but I have the text for them on file) were imported from other classification systems as part of the "Start-up" list that kick started the revision process. It is understood from key ICD documents, that these External Definitions would not display in the final print and electronic versions of ICD-11. All three volumes will be available online. Because the iCAT does not show all the categories, it is not yet evident whether (B)ME will be assigned its own ICD Title Description pages and/or whether (B)ME will be specified as a Synonym to, or Subclass of Gj92 Chronic fatigue syndrome.
The full text for the External Definition that is party visible is:
A syndrome of unknown etiology. Chronic fatigue syndrome (CFS) is a clinical diagnosis characterized by an unexplained persistent or relapsing chronic fatigue that is of at least six months duration, is not the result of ongoing exertion, is not substantially alleviated by rest, and results in substantial reduction of previous levels of occupational, educational, social or personal activities. Common concurrent symptoms of at least six months duration include impairment of memory or concentration, diffuse pain, sore throat, tender lymph nodes,headaches of a new type, pattern, or severity, and nonrestorative sleep. The etiology of CFS may be viral or immunologic. Neurasthenia and fibromyalgia may represent related disorders. Also known as myalgic encephalomyeltis.
Ontology ID UMLS/NC12007_05
E
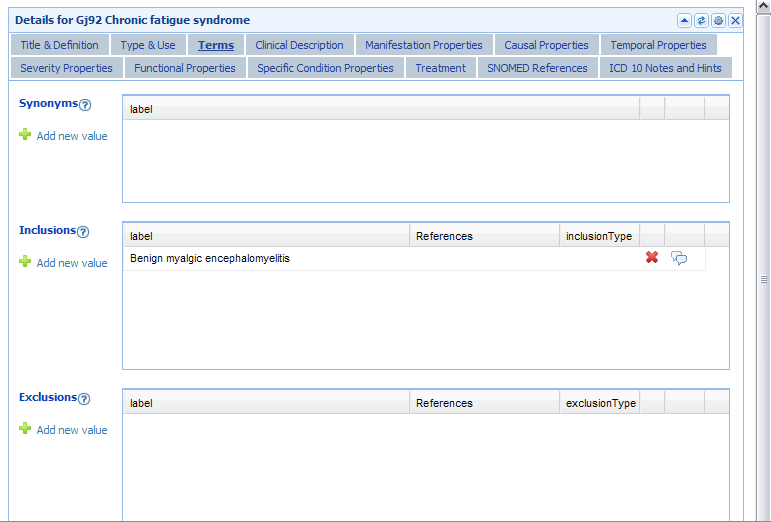
This screenshot shows (B)ME specified as an Inclusion Term to Gj92 Chronic fatigue syndrome:
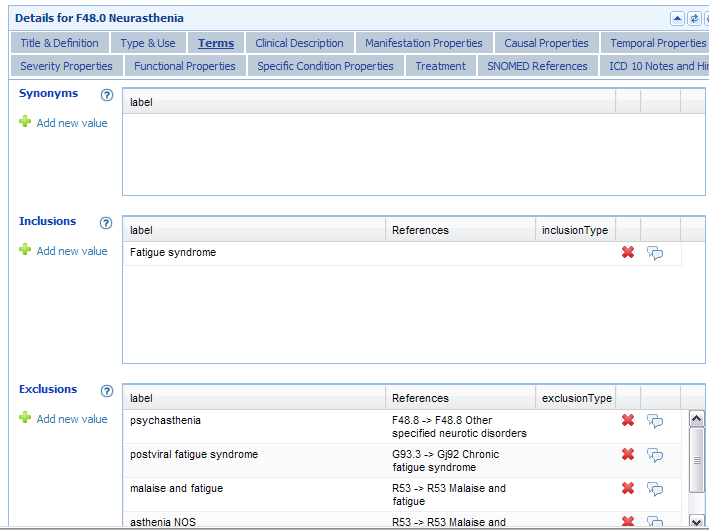
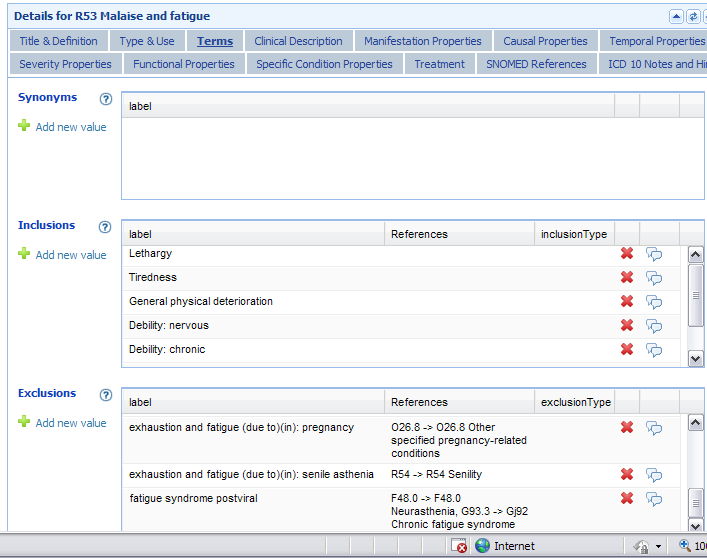
I am including two screenshots from two other ICD-11 Chapters in order to show that "Postviral fatigue syndrome G93.3 -> Gj92 Chronic fatigue syndrome" is specified as an Exclusion to Chapter 5 F48.0 and specified as an Exclusion to R53 Malaise and fatigue (the latter being the R code Chapter 18, where it is proposed to code for Chronic fatigue syndrome NOS in the US specific, ICD-10-CM).
Chapter 5 (V) Somatoform Disorders
Inclusions and Exclusions for Neurasthenia:
Chapter 18 Symptoms and signs
Inclusions and Exclusions for R53 Malaise and fatigue:
The Fields for Synonyms had not been completed at the time these screenshots were made (this was the case for most categories throughout all chapters). But Synonyms, Subclasses etc to ICD Title entities will be specified in ICD-11. Many of the Fields had yet to have their content authored and entered into the iCAT by last year. The sheer amount of textual material to be generated, reviewed and entered into the draft is one of the reasons why the Beta draft targets are slipping.
From the information available, it is not currently possible to determine what the proposed hierarchical status of Postviral fatigue syndrome and Benign myalgic encephalomyelitis will be in relation to Chronic fatigue syndrome, and in relation to each other.
What can be determined, at this point, is that all three terms are proposed to be classified within Chapter 6 and that (B)ME is specified as Inclusion term to CFS.
It may be that PVFS will be subsumed under CFS, as PVFS will be losing its parent code G93, and that CFS will become the ICD Title entity (hence the "Change of hierarchy").
(A request for clarification of these issues was made in late June 2010 to Dr Raad Shakir, Chair, Topic Advisory Group for Neurology, but a response is still awaited at March 2011.)
So to recap, for ICD-11:
All three terms, PVFS, CFS and (Benign) ME are proposed to be classified within Chapter 6 for ICD-11.
"Gj92 Chronic fatigue syndrome" is proposed to be an ICD Title term, with a draft Definition (which may be subject to revision) and with other content fields in the process of being authored and entered into the drafting platform, according to a common "ICD-11 Content Model".
(B)ME is specified under the "Gj92 Chronic fatigue syndrome" Terms parameter as an Inclusion term to Chapter 6 ICD Title term "Gj92 Chronic fatigue syndrome". ("Gj92" is a "Sorting label" not the ICD-11 code.)
"Postviral fatigue syndrome G93.3 -> Gj92 Chronic fatigue syndrome" is specified as an Exclusion to Chapter 5 F48.0 and specified as an Exclusion to Chapter 18 R53 Malaise and fatigue (the latter being the R code, where it is proposed to code for Chronic fatigue syndrome NOS in the US specific, ICD-10-CM).
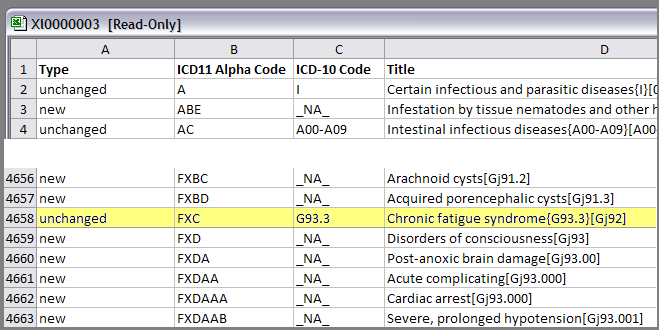
Extract from ICD "DIFF File – Changes from ICD-10" [MS Excel doc. Retrieved 29.09.10; Not available on 01.10.10 as it was taken offline by ICD Revision]
Field “A Type“ specifies: new; unchanged; decision to be made; retired; real retired
[Note: ICD11 Alpha Codes may be temporary sorting codes; "FXC" against "G93.3" does not relate to the F Codes in ICD Chapter 5 (V); note also that Gj92 is an ICD-11 "Sorting label" not an ICD code.]
Extract Spreadsheet:
Extracts from my Dx Revision Watch site June 2010 report:
PVFS, ME, CFS: the ICD-11 Alpha Draft and iCAT Collaborative Authoring Platform: http://wp.me/pKrrB-KK
For full notes that accompany these images, please see the report on my site.
The information in this post relates solely to proposals for ICD-11. It does not apply to ICD-10-CM, the forthcoming US “Clinical Modification” of ICD-10.
There are ICD-10 clinical modifications for ICD-10-AM [Australia], ICD-10-CA [Canada], ICD-10-GM [Germany], ICD-10-TM [Thailand] and ICD-10-CM [United States]. These ICD-10 modifications differ in their number of codes, chapters, and subcategories. Specific conditions are present in some but not all of the modifications.
The most recent release of proposals for ICD-10-CM (release for 2011), both the Index and Tabular List can be downloaded from the CDC site here: http://www.cdc.gov/nchs/icd/icd10cm.htm
ICD-11 screenshots from the iCAT drafting platform
The iCAT drafting platform was taken out of the public domain in November. The platform may be available again, in May, if the Beta Draft is ready by then. ICD Revision has been discussing the pros and cons of postponing the Beta until later this year, or possibly even next year.
Chapter 6 Diseases of the nervous system
Note that existing ICD-10 codings between G83.9 and G99.8 are being reorganised and have been assigned the labels GA thru GN (some of which are parent categories with child and grandchildren categories).
GN Other disorders of the nervous system is a parent to category Gj92 Chronic fatigue syndrome
This iCAT Discussion Note for "Gj92 Chronic fatigue syndrome" records a Change in hierarchy for class: G93.3 Postviral fatigue syndrome because its parent category (G93 Other disorders of brain) is proposed to be removed.
Note that the removal of the parent G93 Other disorders of brain will affect many other categories that were also classified under G93 in ICD-10, not just G93.3.
Note that many categories in the G codes are undergoing reorganisation within Chapter 6 and have been assigned "Sorting labels". It is not known, at this stage, whether PVFS, CFS and ME will be reassigned the G93.3 code because of the reorganisation that is being undertaken within Chapter 6 and because of the removal of the parent term G93.
Note that three External Definitions (which aren't all visible in the screenshot, below, but I have the text for them on file) were imported from other classification systems as part of the "Start-up" list that kick started the revision process. It is understood from key ICD documents, that these External Definitions would not display in the final print and electronic versions of ICD-11. All three volumes will be available online. Because the iCAT does not show all the categories, it is not yet evident whether (B)ME will be assigned its own ICD Title Description pages and/or whether (B)ME will be specified as a Synonym to, or Subclass of Gj92 Chronic fatigue syndrome.
The full text for the External Definition that is party visible is:
A syndrome of unknown etiology. Chronic fatigue syndrome (CFS) is a clinical diagnosis characterized by an unexplained persistent or relapsing chronic fatigue that is of at least six months duration, is not the result of ongoing exertion, is not substantially alleviated by rest, and results in substantial reduction of previous levels of occupational, educational, social or personal activities. Common concurrent symptoms of at least six months duration include impairment of memory or concentration, diffuse pain, sore throat, tender lymph nodes,headaches of a new type, pattern, or severity, and nonrestorative sleep. The etiology of CFS may be viral or immunologic. Neurasthenia and fibromyalgia may represent related disorders. Also known as myalgic encephalomyeltis.
Ontology ID UMLS/NC12007_05
E
This screenshot shows (B)ME specified as an Inclusion Term to Gj92 Chronic fatigue syndrome:
I am including two screenshots from two other ICD-11 Chapters in order to show that "Postviral fatigue syndrome G93.3 -> Gj92 Chronic fatigue syndrome" is specified as an Exclusion to Chapter 5 F48.0 and specified as an Exclusion to R53 Malaise and fatigue (the latter being the R code Chapter 18, where it is proposed to code for Chronic fatigue syndrome NOS in the US specific, ICD-10-CM).
Chapter 5 (V) Somatoform Disorders
Inclusions and Exclusions for Neurasthenia:
Chapter 18 Symptoms and signs
Inclusions and Exclusions for R53 Malaise and fatigue:
The Fields for Synonyms had not been completed at the time these screenshots were made (this was the case for most categories throughout all chapters). But Synonyms, Subclasses etc to ICD Title entities will be specified in ICD-11. Many of the Fields had yet to have their content authored and entered into the iCAT by last year. The sheer amount of textual material to be generated, reviewed and entered into the draft is one of the reasons why the Beta draft targets are slipping.
From the information available, it is not currently possible to determine what the proposed hierarchical status of Postviral fatigue syndrome and Benign myalgic encephalomyelitis will be in relation to Chronic fatigue syndrome, and in relation to each other.
What can be determined, at this point, is that all three terms are proposed to be classified within Chapter 6 and that (B)ME is specified as Inclusion term to CFS.
It may be that PVFS will be subsumed under CFS, as PVFS will be losing its parent code G93, and that CFS will become the ICD Title entity (hence the "Change of hierarchy").
(A request for clarification of these issues was made in late June 2010 to Dr Raad Shakir, Chair, Topic Advisory Group for Neurology, but a response is still awaited at March 2011.)
So to recap, for ICD-11:
All three terms, PVFS, CFS and (Benign) ME are proposed to be classified within Chapter 6 for ICD-11.
"Gj92 Chronic fatigue syndrome" is proposed to be an ICD Title term, with a draft Definition (which may be subject to revision) and with other content fields in the process of being authored and entered into the drafting platform, according to a common "ICD-11 Content Model".
(B)ME is specified under the "Gj92 Chronic fatigue syndrome" Terms parameter as an Inclusion term to Chapter 6 ICD Title term "Gj92 Chronic fatigue syndrome". ("Gj92" is a "Sorting label" not the ICD-11 code.)
"Postviral fatigue syndrome G93.3 -> Gj92 Chronic fatigue syndrome" is specified as an Exclusion to Chapter 5 F48.0 and specified as an Exclusion to Chapter 18 R53 Malaise and fatigue (the latter being the R code, where it is proposed to code for Chronic fatigue syndrome NOS in the US specific, ICD-10-CM).
Extract from ICD "DIFF File – Changes from ICD-10" [MS Excel doc. Retrieved 29.09.10; Not available on 01.10.10 as it was taken offline by ICD Revision]
Field “A Type“ specifies: new; unchanged; decision to be made; retired; real retired
[Note: ICD11 Alpha Codes may be temporary sorting codes; "FXC" against "G93.3" does not relate to the F Codes in ICD Chapter 5 (V); note also that Gj92 is an ICD-11 "Sorting label" not an ICD code.]
Extract Spreadsheet:
